
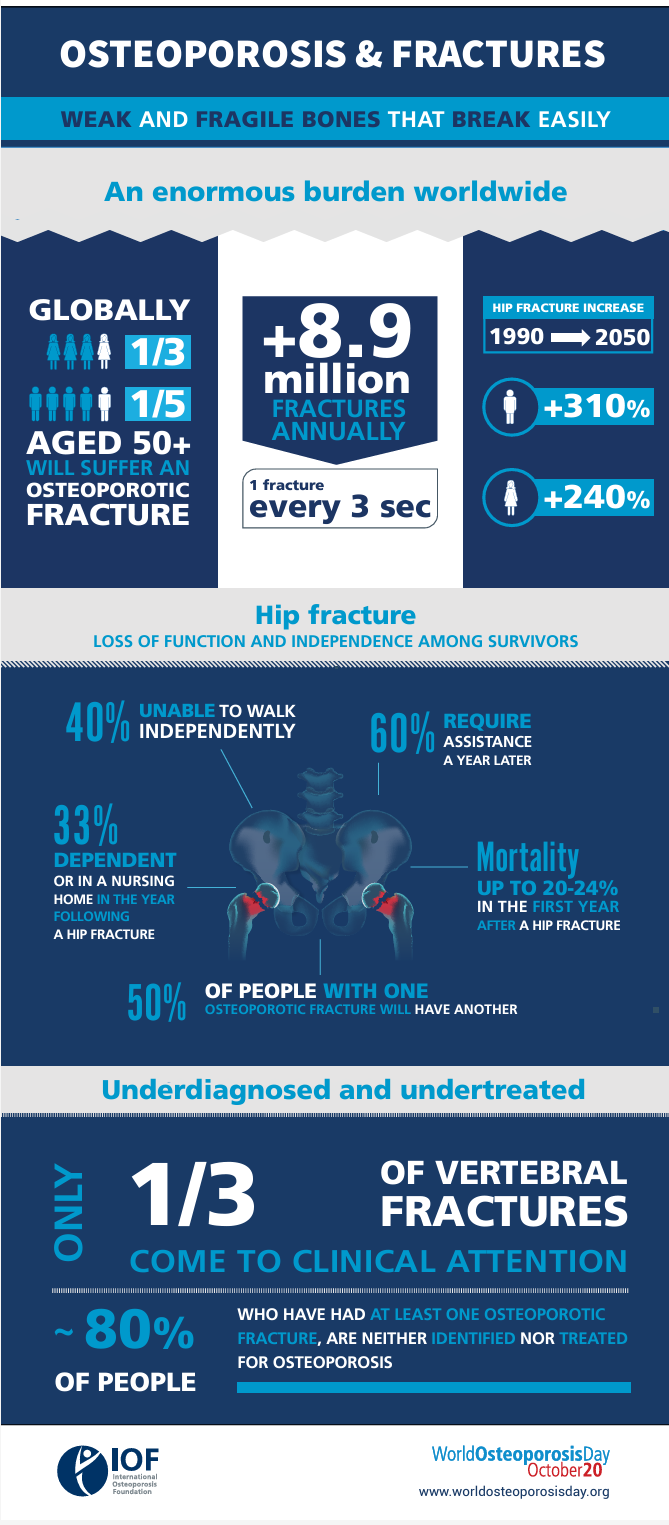
Building and maintaining bone mass is a big deal with 1 in 5 females and 1 in 20 men over the age of 50 showing signs of osteoporosis [1]. Bone mineral density seems to decline at a rate of 0.6% to 2.1% per year after the age of 60 without fighting gravity through resistance training [2]. According to the CDC, as high as 1 in 3 older adults will experience a fall each year, and over 1 in 3 of those falls will likely require medical attention. Currently, an estimated 300,000 hip fractures occur in the US each year which increases one’s risk of death for the subsequent year and one is never really out of the clear as this increased risk is seemingly still there 20 years after a fall [1].
It appears that resistance training may be able to increase bone mineral density (BMD) at a rate similar to pharmacological means [3, 4]. Furthermore, resistance training and medications may have an additive or even synergistic effect [5]. It appears that higher-intensity resistance training may be more effective for stimulating bone adaptations [6, 7].
The precision error for BMD measured via dual-energy X-ray absorptiometry (DEXA) can be close to the rate of increase or decline that one might see from annual aging or from the interventions listed above [8, 9]. Therefore, one would likely want to see an improvement beyond 1-2% to know that they overwhelmed the technical error of the device and operator. This metric could be tracked annually or every other year ideally utilizing the same positioning and scanning facility.
You have probably already heard about and seen all kinds of infographics about bone loss without resistance training. This story is pervasive in the fitness world. We love to yell about old people falling down and breaking their hips.
Perhaps, repeating the salience of outcomes story on this topic can be helpful for behavior change and getting people in the weight room. The effect size is there and prevention over the life course looks to be possible.
Another aspect that may be helpful for reducing osteoporosis risk later in life is attaining as much bone as possible in one’s youth [10]. This is referred to as peak bone mass. Some factors that seem to influence peak bone mass are ethnicity, smoking, alcohol consumption, nutrition intake, and sport and resistance training participation [11, 12]. Thus, resistance training, exercise, and sports performance while providing adequate nutrition during this period may help an individual build a larger chassis.
As would be expected, athletes across a multitude of sports (except swimming) and age ranges look to have higher bone mineral density than non-exercising control populations [13-16]. Additionally, frame size seems to correlate with measures of Fat-Free Mass (FFM) and Bone Mineral Content (BMC) and maybe BMC explains a small percentage of the variation in FFM in the general population [17, 18].
Higher amounts of bone and frame size seem to be related to overall skeletal muscle mass, but the relationship is not as definitive as the internet would lead us to believe and we need more research in this area to establish if one can in any way predict an individual’s max muscular potential based on their bone mass. Furthermore, although exercise interventions can increase bone later in life in untrained populations we also need more research to assess if novice or advanced trainees can increase their bone mass over longer periods of time in their 20s and 30s through resistance training and/or participation in sport.
There is an urban legend that one can hold five pounds of muscle for every pound of bone. This hypothesis is based on anthropometric metric equations from thesis-level research of cadavers that were performed in the 1980s [19, 20], and the body fat percentages and bone metrics from these specific equations have not been or do not seem to significantly correlate with newer age testing like DEXA and magnetic resonance imaging (MRI) [21, 22]. This is not to say these type of methods [23, 24] are not accurate or useful, but further validation and replication is needed [22].
Dengel and colleagues [13] recently looked at the muscle-to-bone ratio (MBR) measured via DEXA in NFL athletes in comparison to healthy aged-matched controls. They found that the NFL players had significantly more lean mass and bone mineral content and a lower body fat percentage, but a lower total muscle-to-bone ratio (MBR) compared to the health age-matched controls. “This is due to the fact that the NFL players were taller, resulting in a larger total skeleton and ultimately a greater amount of BMC for a proportional amount of lean mass resulting in lower total MBR. Although we found differences between professional football players and a control population, no positional differences in total MBR in the NFL athletes were observed.”
The MBR values from this study are also around 4 to 5 times higher than previous studies that have utilized anthropometric measurements and equations to estimate MBRs. This is likely due to the differences in wet vs. dry bone mass. Of note, the anthropometric equations seem to be operating on the assumption that the ratio of dry to wet bone mass is constant, but this does not look to be the case.
To finish this off, let’s take a look at DEXA results from myself and coach Ryan L’Ecuyer to see how they compare to the football study above. My most recent DEXA at the end of a lean gain phase had me at 12.1% body fat and 177.2 lb. This equals an FFMI of around 23 and if I took the governor off fat accumulation as I have done in the past this FFMI would likely push into the 24 to 24.5 range. Following the same methods as Dengel and colleagues my MBR was 21.7. This MBR is higher than the average of 18.5 across all the NFL athletes. This is interesting as the average FFMI in this study for the lineman was 26.5 to 27.3, the running backs were 26.5, and the DBs and wide receivers were between 23.5 and 24. This is surprising and if I wanted to make up an interesting conjecture off extremely limited data with different DEXA scanners I would posit that the NFL players could likely gain more muscle mass in specific less trained regions by transitioning to a pure hypertrophy program. Just out of curiosity, I also put in the DEXA results from the NFL athletes I have in our system and the MBRs were all between 17 and 19.
As we have discussed before Ryan has one of the highest lifetime natural FFMIs we have ever seen at roughly 30.5 on a Lunar iDXA and his MBR is 20.5. I have DEXAs from a few other meat monsters with FFMIs >26 and they are all above 20 on an MBR. Furthermore, I asked Dr. Grant Tinsley for the BMC data from a cross-sectional study on body composition in quite developed bodybuilders (~59% of which reported current or previous anabolic use) that was published in 2020 [25]. The average FFMI from the DEXA for the males in this study was 25.3 and the MBR for the males was 22.0 ± 1.3. In comparison, case studies of all-natural male bodybuilders have MBRs in the 23-24 range [26] and 18-19 for females [27]. There was also a sumo wrestler study published in 2022 and it seems that if there is no cap on fat accumulation the middle weights hit an MBR of 23.4 and the heavy weights were the highest natural values I have seen thus far at 24.9 [28].
TL;DR - Bone is important and BMD will decrease significantly as we age without exercise. It appears that bone mass can be increased and maintained throughout the life course, but we do not know if highly trained individuals can increase their bone mass and if this increase would in some way permit an increase in muscular potential. Peak bone mass is important for the prevention of osteoporosis and we can hypothesize that peak bone mass may also be related to one's peak muscular potential. Someone's MBR may be a way to further extrapolate how close someone is to their maximal muscular potential, but more research is needed.
REFERENCES:
1. Neda Sarafrazi, P.D., Edwina A. Wambogo, Ph.D., M.S., M.P.H., R.D., and John A. Shepherd, Ph.D. Osteoporosis or Low Bone Mass in Older Adults: United States, 2017–2018. 2021.
2. Gomez-Cabello, A., et al., Effects of training on bone mass in older adults: a systematic review. Sports Med, 2012. 42(4): p. 301-25.
3. Massini, D.A., et al., The Effect of Resistance Training on Bone Mineral Density in Older Adults: A Systematic Review and Meta-Analysis. Healthcare (Basel), 2022. 10(6).
4. Berry, S.D., et al., Changes in bone mineral density (BMD): a longitudinal study of osteoporosis patients in the real-world setting. Arch Osteoporos, 2018. 13(1): p. 124.
5. Kistler-Fischbacher, M., et al., A Comparison of Bone-Targeted Exercise With and Without Antiresorptive Bone Medication to Reduce Indices of Fracture Risk in Postmenopausal Women With Low Bone Mass: The MEDEX-OP Randomized Controlled Trial. J Bone Miner Res, 2021. 36(9): p. 1680-1693.
6. Kitagawa, T., et al., A comparison of different exercise intensities for improving bone mineral density in postmenopausal women with osteoporosis: A systematic review and meta-analysis. Bone Rep, 2022. 17: p. 101631.
7. Zamoscinska, M., I.R. Faber, and D. Busch, Do Older Adults With Reduced Bone Mineral Density Benefit From Strength Training? A Critically Appraised Topic. J Sport Rehabil, 2020. 29(6): p. 833-840.
8. Kiebzak, G.M., et al., Effect of precision error on T-scores and the diagnostic classification of bone status. J Clin Densitom, 2007. 10(3): p. 239-43.
9. Hind, K., B. Oldroyd, and J.G. Truscott, In vivo precision of the GE Lunar iDXA densitometer for the measurement of total-body, lumbar spine, and femoral bone mineral density in adults. J Clin Densitom, 2010. 13(4): p. 413-7.
10. Chevalley, T. and R. Rizzoli, Acquisition of peak bone mass. Best Pract Res Clin Endocrinol Metab, 2022. 36(2): p. 101616.
11. Zhu, X. and H. Zheng, Factors influencing peak bone mass gain. Front Med, 2021. 15(1): p. 53-69.
12. Behringer, M., et al., Effects of weight-bearing activities on bone mineral content and density in children and adolescents: a meta-analysis. J Bone Miner Res, 2014. 29(2): p. 467-78.
13. Dengel, D.R. and N.G. Evanoff, Positional Differences in Muscle-to-bone Ratio in National Football League Players. Int J Sports Med, 2023. 44(10): p. 720-727.
14. Stojanovic, E., et al., Basketball players possess a higher bone mineral density than matched non-athletes, swimming, soccer, and volleyball athletes: a systematic review and meta-analysis. Arch Osteoporos, 2020. 15(1): p. 123.
15. Kopiczko, A., et al., Bone mineral density in elite masters athletes: the effect of body composition and long-term exercise. Eur Rev Aging Phys Act, 2021. 18(1): p. 7.
16. Antonio, J., et al., Bone Mineral Density in Competitive Athletes. 2018.
17. Chumlea, W.C., et al., Relations between frame size and body composition and bone mineral status. Am J Clin Nutr, 2002. 75(6): p. 1012-6.
18. Evans, E.M., et al., Relation of bone mineral density and content to mineral content and density of the fat-free mass. J Appl Physiol (1985), 2001. 91(5): p. 2166-72.
19. Kerr, An anthropometric method for fractionation of skin, adipose, bone, muscle and residual tissue masses in males and females age 6 to 77 years. 1988.
20. Martin, An anatomical basis for assessing human body composition : evidence from 25 dissections. 1984.
21. Gonzalez-Mendoza, R.G., et al., Accuracy of Anthropometric Equations to Estimate DXA-Derived Skeletal Muscle Mass in Professional Male Soccer Players. J Sports Med (Hindawi Publ Corp), 2019. 2019: p. 4387636.
22. Kasper, A.M., et al., Come Back Skinfolds, All Is Forgiven: A Narrative Review of the Efficacy of Common Body Composition Methods in Applied Sports Practice. Nutrients, 2021. 13(4).
23. Menargues-Ramirez, R., et al., Evaluation of Body Composition in CrossFit((R)) Athletes and the Relation with Their Results in Official Training. Int J Environ Res Public Health, 2022. 19(17).
24. Bernal-Orozco, M.F., et al., Anthropometric and Body Composition Profile of Young Professional Soccer Players. J Strength Cond Res, 2020. 34(7): p. 1911-1923.
25. Graybeal, A.J., et al., Body Composition Assessment in Male and Female Bodybuilders: A 4-Compartment Model Comparison of Dual-Energy X-Ray Absorptiometry and Impedance-Based Devices. J Strength Cond Res, 2020. 34(6): p. 1676-1689.
26. Kistler, B.M., et al., Case study: Natural bodybuilding contest preparation. Int J Sport Nutr Exerc Metab, 2014. 24(6): p. 694-700.
27. Newmire, D.E. and H.E. Webb, The role of age in the physiological adaptations and psychological responses in bikini-physique competitor contest preparation: a case series. J Int Soc Sports Nutr, 2021. 18(1): p. 45.
28. Midorikawa, T., et al., Characteristics of total body and appendicular bone mineral content and density in Japanese collegiate Sumo wrestlers. Sci Rep, 2022. 12(1): p. 11796.



Related Content
Can You Trust Bioimpedance To Measure Your Body Fat Percentage?
Mar 28, 2026
The Muscle To Bone Ratio Revisited
Mar 17, 2026
Revisiting Diet-Induced Muscle Loss.
Feb 14, 2026