

It appears that the oral testosterone (testosterone undecanoate) options are 84 to 88% effective in getting hypogonadal men back into the normal range of testosterone [1-4]. This can get into the high 90% range with dose titrations [5]. All of the clinical trials referenced above have tested oral testosterone against a gel or no comparator, and the oral derivatives seem to perform just as well or better for the majority of the other sexual health, psychological, and safety outcomes. To the best of my knowledge, there is currently no study that has compared an oral testosterone option to an injectable form of testosterone.
As we have discussed previously, the half-life of injectable testosterone varieties is roughly between 2 and 8 days, depending on the compound. Whereas, the oral medications have a half-life of roughly 3-4 hours and peak at 4 to 6 hours after ingestion. Thus, these oral options are going to have more swings in testosterone concentrations throughout the day, and depending on the dose, very very likely have lower overall total area under the curve values for testosterone.
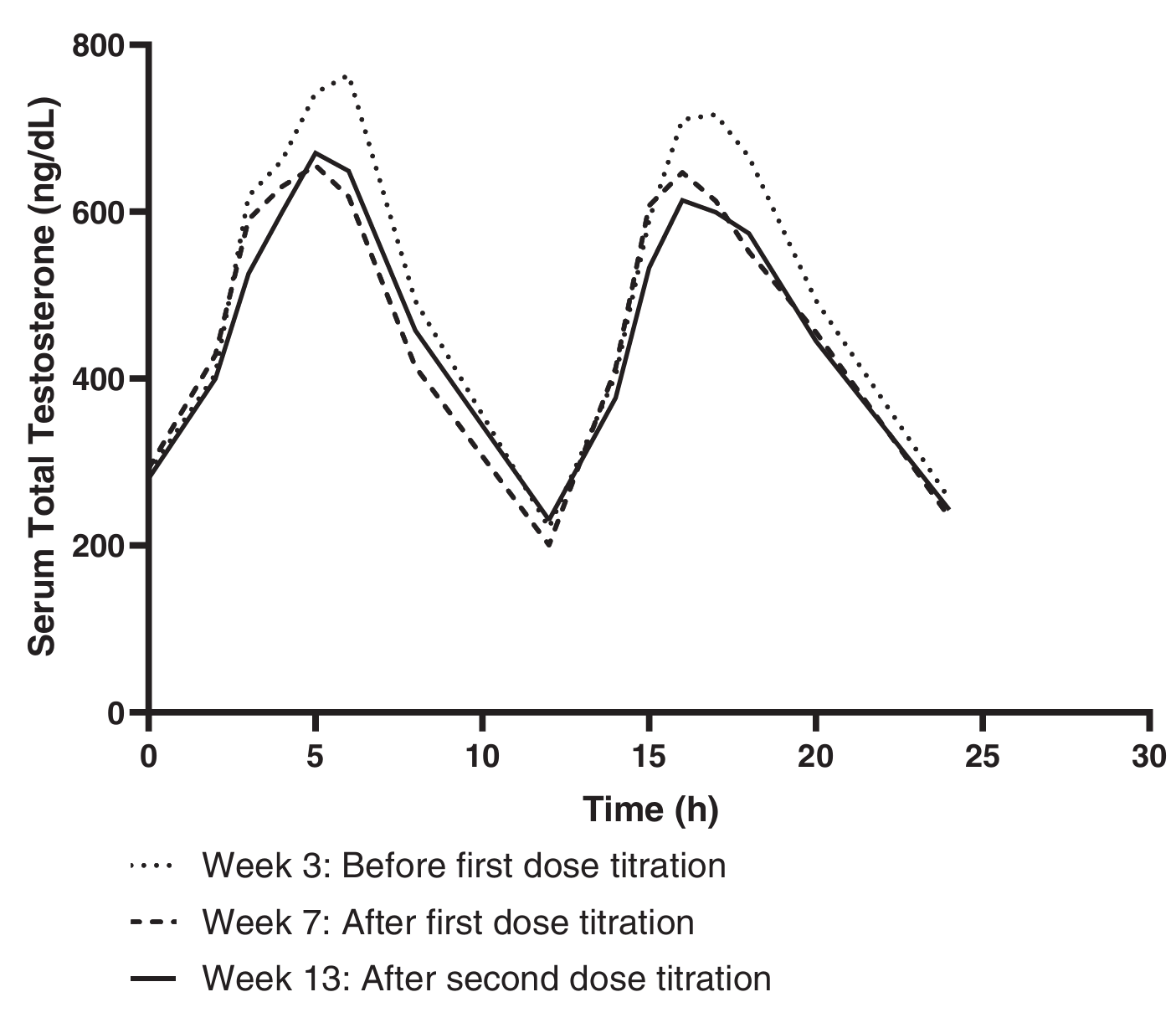
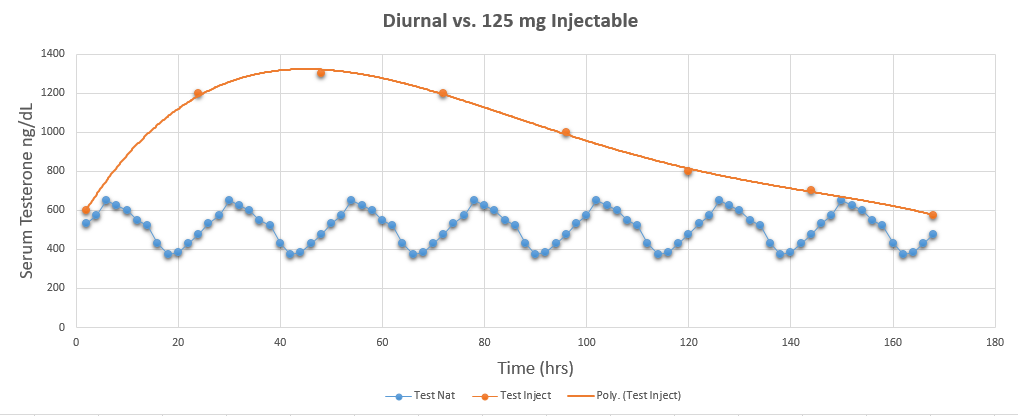
You can see in the twice-daily oral testosterone dosage above that serum testosterone values are falling into the hypogonadal range twice over a 24-hour period, but this double peak is more akin to the natural diurnal variation in testosterone that you see depicted in blue below over 180 hours. In a weekly or biweekly injectable dosage, testosterone values are theoretically never falling into the hypogonadal range, and the peak is likely almost double that of the oral forms at the current dosing.
It may be possible to keep levels more even with more frequent dosing of the oral derivatives just like you see being done over longer time frames with the injectables. This is likely a balance between the subjective advantage of more stable levels and the burden and potential decrease in consistency from having to inject or take a pill more often. It is also important to note that the oral options are likely better absorbed with a higher fat meal (20 to 45 grams), which logistically likely maxes the frequency out at 3 to 4 times per day.
To date, there is only one poster abstract that has investigated the body composition changes from these oral derivatives in hypogonadal males [6]. They found that after 180 days, fat mass decreased by 1.9 ± 2.8 kg and lean body mass increased by 2.9 ± 2.7 kg measured via DEXA. At one year, fat mass had decreased by an additional 0.5 kg, and lean body mass had increased by an additional 0.3 kg, but this was very likely not significantly different from 180 days. The researchers do not report a p-value between 180 and 365 days. Bone mineral density also showed statistically significant minor improvements during this time frame. We have covered the potential muscle gain from other TRT formulations HERE.
Given the area under the curve for the oral derivatives, I would not really expect a male who is borderline low-normal in testosterone to gain any appreciable amount of lean body mass or contractile tissue from this type of dosing pattern. If eugonadal males are given this type of testosterone at TRT dosages, a significant decrease in testosterone has been observed [7]. That is all I will say on that, as you can get my full sentiments about flippant TRT+ initiation from the Iron Culture podcast HERE. It is also important to note that this type of testosterone could result in an increase in blood pressure and hematocrit that should be adequately monitored by the prescribing physician [8].
A reminder that someone can gain muscle even if they "have low T", and gaining muscle and simultaneously losing fat could increase testosterone in an overweight or obese population HERE and HERE. That said, if a male is truly hypogonadal, TRT is efficacious on a variety of fronts and may aid in improving muscle, bone, metabolic, and psychosexual health.
REFERENCES:
1. DelConte, A., et al., A new oral testosterone (TLANDO) treatment regimen without dose titration requirement for male hypogonadism. Andrology, 2022. 10(4): p. 669-676.
2. Miner, M., et al., Safety, efficacy, and pharmacokinetics of oral testosterone undecanoate in males with hypogonadism. Andrology, 2025. 13(4): p. 882-893.
3. Bernstein, J.S. and O.P. Dhingra, A phase III, single-arm, 6-month trial of a wide-dose range oral testosterone undecanoate product. Ther Adv Urol, 2024. 16: p. 17562872241241864.
4. Swerdloff, R.S. and R.E. Dudley, A new oral testosterone undecanoate therapy comes of age for the treatment of hypogonadal men. Ther Adv Urol, 2020. 12: p. 1756287220937232.
5. Swerdloff, R.S., et al., A New Oral Testosterone Undecanoate Formulation Restores Testosterone to Normal Concentrations in Hypogonadal Men. J Clin Endocrinol Metab, 2020. 105(8): p. 2515-31.
6. Swerdloff, R.S., et al., SAT-044 Treatment of Hypogonadal Men with a New Oral Testosterone Undecanoate (TU) Formulation Improves Psychosexual, Well-Being and Body Composition and Bone Density Parameters. Journal of the Endocrine Society, 2020. 4(Supplement_1).
7. Miller, J.A., et al., Oral testosterone therapy: past, present, and future. Sex Med Rev, 2023. 11(2): p. 124-138.
8. Nackeeran, S., et al., The Effect of Route of Testosterone on Changes in Hematocrit: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Trials. J Urol, 2022. 207(1): p. 44-51.




Related Content
What Would It Take To Really Map Out The Androgen Signaling Network?
Jan 23, 2026
How Does Sleep and Sleep Loss Affect Testosterone?
Dec 05, 2025
How Much Does Androgen Receptor Sensitivity Matter?
Nov 16, 2025