

Dehydroepiandrosterone (DHEA) is a hormone produced by the adrenal glands that is available over the counter in the US. It is still a WADA-banned substance, but does it actually increase muscle mass, lowr fat mass, or significantly increase strength?
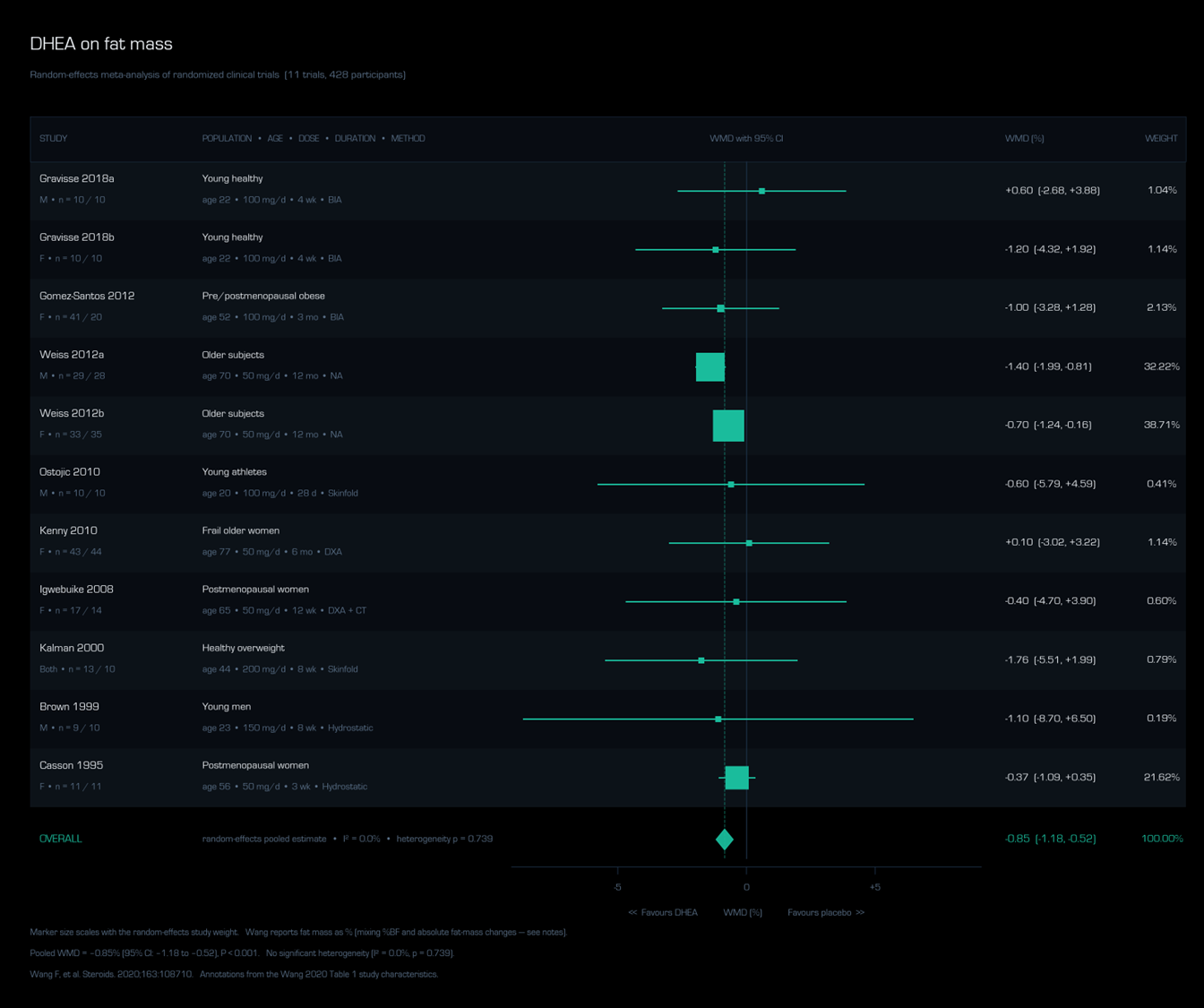
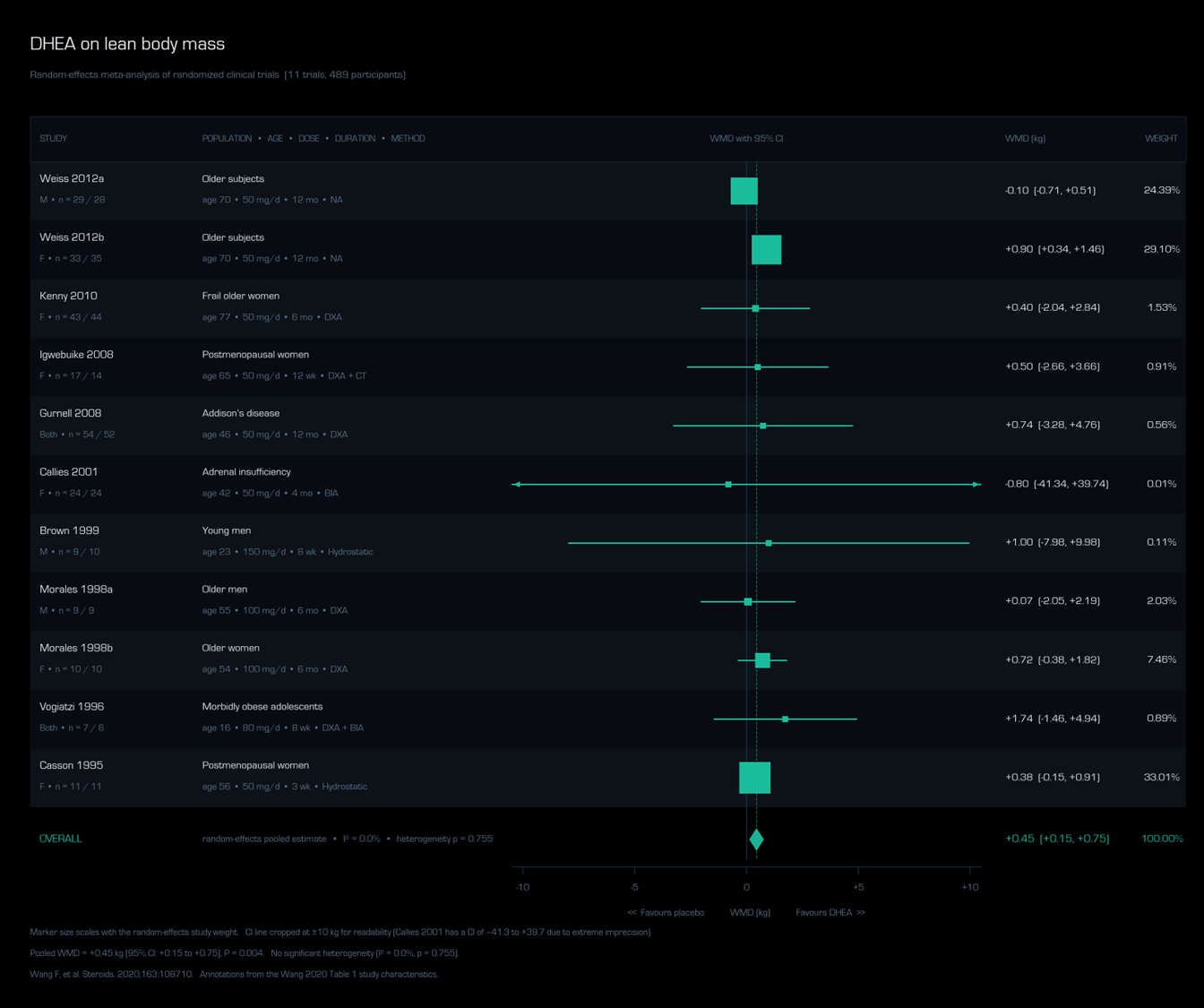
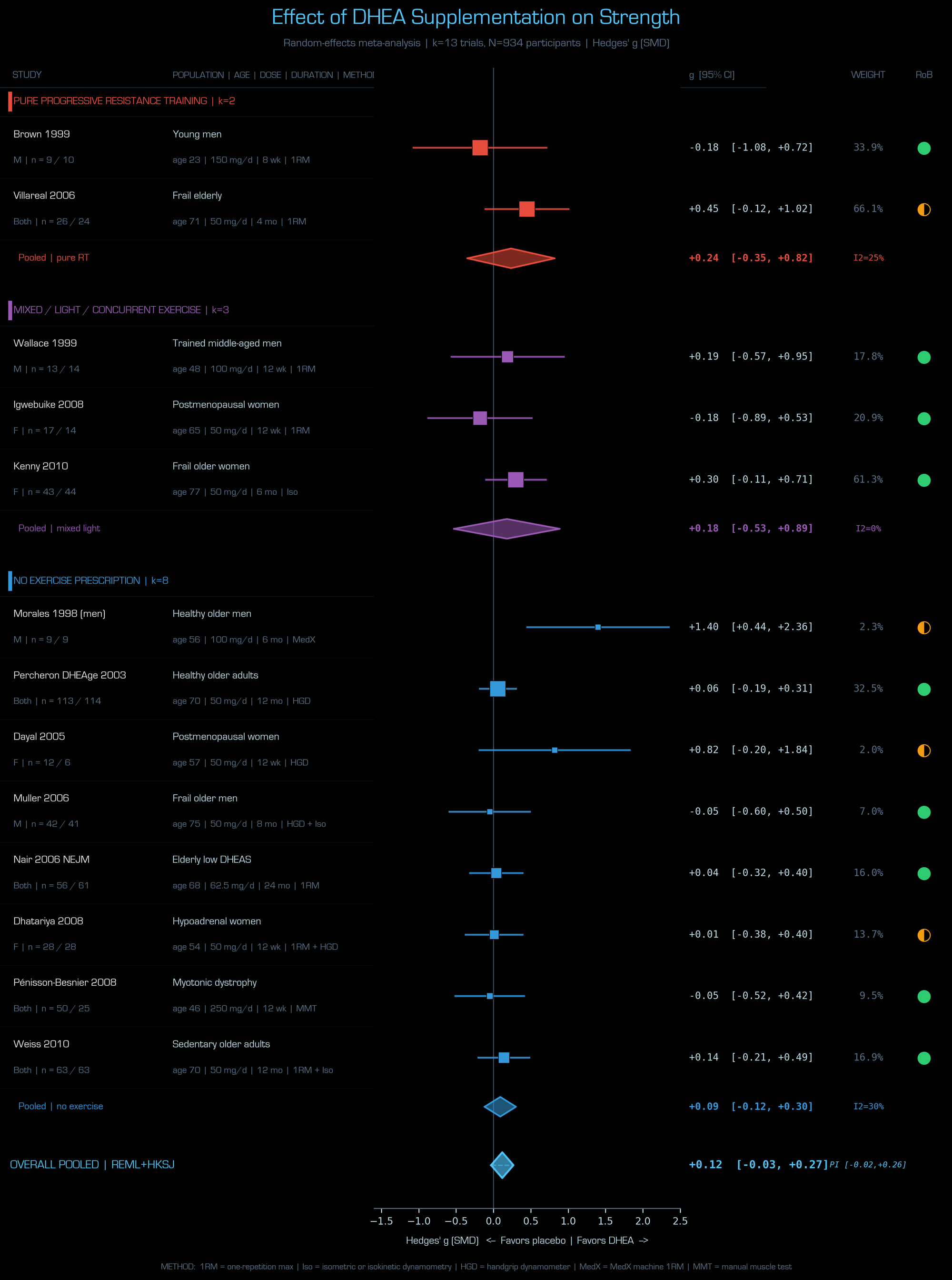
TL;DW - There might be a little, maybe something there on the body composition side. Any signal is likely coming from older individuals, and there is unlikely to be a benefit in young healthy subjects. There has not been a published meta-analysis on strength. It will very likely be null.
Below is a scorched-earth deep dive into what can and can't affect DHEA and what supplementing what else DHEA may and may not move the needle on:
Briefly, there are some very serious medical conditions that can bottom out DHEA-S. High allostatic load and fatty liver also seem to reduce it and these are inherently intertwined, as many of the allostatic load calculators subtly capture metabolic health. DHEA-S also appears to decrease with age. Sleep deprivation, fragmentation, and OSA don't seem to do much and sleep extension doesn't seem to increase it. Also, with limited data, DHEA-S doesn't appear to be a reliable marker of overtraining syndrome. Regular physical activity in older adults and mindfulness-based stress reduction may somewhat increase it.
DHEA-S / Modulators
A consolidated map of what raises, lowers, and fails to move circulating DHEA-S — and what supplementing it actually accomplishes. Magnitudes from RCTs, meta-analyses, and Mendelian randomization where available. Sex stratifies many findings dramatically.
What Lowers DHEA-S in Men
↓ SuppressorsWhat Doesn't Reliably Lower It
≈ ResilientWhat Raises Endogenous DHEA-S
↑ InterventionsDHEA Supplementation in Men
⚖ OutcomesPossibly Helpful
Mixed / Modest
Doesn't Improve
Cautions
What Lowers DHEA-S in Women
↓ SuppressorsWhat Doesn't Reliably Lower It
≈ ResilientWhat Raises Endogenous DHEA-S
↑ InterventionsDHEA Supplementation in Women
⚖ OutcomesReliably Improves
Mixed / Modest
Doesn't Improve
Adverse / Caution
REFERENCES FOR DHEA FOREST PLOTS:
1. Wang, F., et al., The effects of dehydroepiandrosterone (DHEA) supplementation on body composition and blood pressure: a meta-analysis of randomized clinical trials. Steroids, 2020. 163: p. 108710.
2. Brown, G.A., et al., Effect of oral DHEA on serum testosterone and adaptations to resistance training in young men. J Appl Physiol (1985), 1999. 87(6): p. 2274–83.
3. Dayal, M., et al., Supplementation with DHEA: effect on muscle size, strength, quality of life, and lipids. J Womens Health (Larchmt), 2005. 14(5): p. 391–400.
4. Dhatariya, K.K., et al., Dehydroepiandrosterone replacement therapy in hypoadrenal women: protein anabolism and skeletal muscle function. Mayo Clin Proc, 2008. 83(11): p. 1218–25.
5. Igwebuike, A., et al., Lack of dehydroepiandrosterone effect on a combined endurance and resistance exercise program in postmenopausal women. J Clin Endocrinol Metab, 2008. 93(2): p. 534–8.
6. Kenny, A.M., et al., Dehydroepiandrosterone combined with exercise improves muscle strength and physical function in frail older women. J Am Geriatr Soc, 2010. 58(9): p. 1707–14.
7. Morales, A.J., et al., The effect of six months treatment with a 100 mg daily dose of dehydroepiandrosterone (DHEA) on circulating sex steroids, body composition and muscle strength in age-advanced men and women. Clin Endocrinol (Oxf), 1998. 49(4): p. 421–32.
8. Muller, M., et al., Effects of dehydroepiandrosterone and atamestane supplementation on frailty in elderly men. J Clin Endocrinol Metab, 2006. 91(10): p. 3988–91.
9. Nair, K.S., et al., DHEA in elderly women and DHEA or testosterone in elderly men. N Engl J Med, 2006. 355(16): p. 1647–59.
10. Pénisson-Besnier, I., et al., Dehydroepiandrosterone for myotonic dystrophy type 1. Neurology, 2008. 71(6): p. 407–12.
11. Percheron, G., et al., Effect of 1-year oral administration of dehydroepiandrosterone to 60- to 80-year-old individuals on muscle function and cross-sectional area: a double-blind placebo-controlled trial. Arch Intern Med, 2003. 163(6): p. 720–7.
12. Villareal, D.T. and J.O. Holloszy, DHEA enhances effects of weight training on muscle mass and strength in elderly women and men. Am J Physiol Endocrinol Metab, 2006. 291(5): p. E1003–8.
13. Wallace, M.B., et al., Effects of dehydroepiandrosterone vs androstenedione supplementation in men. Med Sci Sports Exerc, 1999. 31(12): p. 1788–92.
14. Weiss, E.P., D.T. Villareal, and J.O. Holloszy, Effect of DHEA replacement therapy on muscle strength and size in sedentary older adults. Med Sci Sports Exerc, 2010. 42(5 Suppl): Abstract 590 (presented at ACSM Annual Meeting, June 2, 2010, Baltimore, MD).
REFERENCES FOR DHEA TABLE:
1. Yasinska, V., et al., Low levels of endogenous anabolic androgenic steroids in females with severe asthma taking corticosteroids. ERJ Open Res, 2023. 9(5): p. 00269-2023.
2. Gurnell, E.M., et al., Long-term DHEA replacement in primary adrenal insufficiency: a randomized, controlled trial. J Clin Endocrinol Metab, 2008. 93(2): p. 400–9.
3. Daniell, H.W., Hypogonadism in men consuming sustained-action oral opioids. J Pain, 2002. 3(5): p. 377–84.
4. Rubinstein, A.L., et al., Association between commonly prescribed opioids and androgen deficiency in men: a retrospective cohort analysis. Pain Med, 2017. 18(4): p. 637–44.
5. Beishuizen, A., et al., Decreased levels of dehydroepiandrosterone sulphate in severe critical illness: a sign of exhausted adrenal reserve?. Crit Care, 2002. 6(5): p. 434–8.
6. Bentley, C., et al., Dehydroepiandrosterone: a potential therapeutic agent in the treatment and rehabilitation of the traumatically injured patient. Burns Trauma, 2019. 7: p. 26.
7. Corona, G., et al., Dehydroepiandrosterone supplementation in elderly men: a meta-analysis study of placebo-controlled trials. J Clin Endocrinol Metab, 2013. 98(9): p. 3615–26.
8. Nair, K.S., et al., DHEA in elderly women and DHEA or testosterone in elderly men. N Engl J Med, 2006. 355(16): p. 1647–59.
9. Charlton, M., et al., Low circulating levels of dehydroepiandrosterone in histologically advanced nonalcoholic fatty liver disease. Hepatology, 2008. 47(2): p. 484–92.
10. Kannisto, S., et al., Serum dehydroepiandrosterone sulfate concentration as an indicator of adrenocortical suppression during inhaled steroid therapy in adult asthmatic patients. Eur J Endocrinol, 2004. 150(5): p. 687–90.
11. Dessein, P.H., et al., Hyposecretion of the adrenal androgen dehydroepiandrosterone sulfate and its relation to clinical variables in inflammatory arthritis. Arthritis Res, 2001. 3(3): p. 183–8.
12. Arlt, W., et al., Oral dehydroepiandrosterone for adrenal androgen replacement: pharmacokinetics and peripheral conversion to androgens and estrogens in young healthy females after dexamethasone suppression. J Clin Endocrinol Metab, 1998. 83(6): p. 1928–34.
13. Jankowski, C.M., et al., Sex-specific effects of dehydroepiandrosterone (DHEA) on bone mineral density and body composition: a pooled analysis of four clinical trials. Clin Endocrinol (Oxf), 2019. 90(2): p. 293–300.
14. von Mühlen, D., et al., Effect of dehydroepiandrosterone supplementation on bone mineral density, bone markers, and body composition in older adults: the DAWN trial. Osteoporos Int, 2008. 19(5): p. 699–707.
15. Lin, H., et al., A systematic review and meta-analysis of randomized placebo-controlled trials of DHEA supplementation of bone mineral density in healthy adults. Gynecol Endocrinol, 2019. 35(11): p. 924–31.
16. Quester, J., et al., Endogenous DHEAS is causally linked with lumbar spine bone mineral density and forearm fractures in women. J Clin Endocrinol Metab, 2022. 107(5): p. e2080–6.
17. He, S., et al., Impact of DHEA supplementation on testosterone and estradiol levels in postmenopausal women: a meta-analysis of randomized controlled trials assessing dose and duration effects. Diabetol Metab Syndr, 2025. 17(1): p. 258.
18. Jørgensen, M.A., et al., Effect of Mindfulness-Based Stress Reduction on dehydroepiandrosterone-sulfate in adults with self-reported stress. A randomized trial. Clin Transl Sci, 2021. 14(6): p. 2360–9.
19. Wang, F., et al., The effects of dehydroepiandrosterone (DHEA) supplementation on body composition and blood pressure: a meta-analysis of randomized clinical trials. Steroids, 2020. 163: p. 108710.
20. Dhatariya, K., et al., Effect of dehydroepiandrosterone replacement on insulin sensitivity and lipids in hypoadrenal women. Diabetes, 2005. 54(3): p. 765–9.
21. Brown, G.A., et al., Effect of oral DHEA on serum testosterone and adaptations to resistance training in young men. J Appl Physiol (1985), 1999. 87(6): p. 2274–83.
22. Wallace, M.B., et al., Effects of dehydroepiandrosterone vs androstenedione supplementation in men. Med Sci Sports Exerc, 1999. 31(12): p. 1788–92.
23. Labrie, F., et al., Effect of intravaginal prasterone on sexual dysfunction in postmenopausal women with vulvovaginal atrophy. J Sex Med, 2015. 12(12): p. 2401–12.
24. Lemos, M.J., et al., Intravaginal dehydroepiandrosterone for the treatment of vulvovaginal atrophy: a systematic review and meta-analysis. Menopause, 2026.
25. Panjari, M., et al., A randomized trial of oral DHEA treatment for sexual function, well-being, and menopausal symptoms in postmenopausal women with low libido. J Sex Med, 2009. 6(9): p. 2579–90.
26. Elraiyah, T., et al., Clinical review: the benefits and harms of systemic dehydroepiandrosterone (DHEA) in postmenopausal women with normal adrenal function: a systematic review and meta-analysis. J Clin Endocrinol Metab, 2014. 99(10): p. 3536–42.
27. Wierman, M.E., et al., Should dehydroepiandrosterone be administered to women?. J Clin Endocrinol Metab, 2022. 107(6): p. 1679–85.
28. Scheffers, C.S., et al., Dehydroepiandrosterone for women in the peri- or postmenopausal phase. Cochrane Database Syst Rev, 2015. 1(1): p. CD011066.
29. Kritz-Silverstein, D., et al., Effects of dehydroepiandrosterone supplementation on cognitive function and quality of life: the DHEA and Well-Ness (DAWN) trial. J Am Geriatr Soc, 2008. 56(7): p. 1292–8.
30. DiVasta, A.D., et al., The effect of gonadal and adrenal steroid therapy on skeletal health in adolescents and young women with anorexia nervosa. Metabolism, 2012. 61(7): p. 1010–20.
31. Lin, J., et al., Dehydroepiandrosterone status and efficacy of dehydroepiandrosterone supplementation for bone health in anorexia nervosa: a systematic review and meta-analysis. Int J Eat Disord, 2022. 55(6): p. 733–46.
32. Cadegiani, F.A., et al., Hormonal aspects of overtraining syndrome: a systematic review. BMC Sports Sci Med Rehabil, 2017. 9: p. 14.
33. Cadegiani, F.A., et al., Basal hormones and biochemical markers as predictors of overtraining syndrome in male athletes: the EROS-BASAL study. J Athl Train, 2019. 54(8): p. 906–14.
34. Villareal, D.T., et al., Effect of DHEA on abdominal fat and insulin action in elderly women and men: a randomized controlled trial. JAMA, 2004. 292(18): p. 2243–8.
35. Alkatib, A.A., et al., A systematic review and meta-analysis of randomized placebo-controlled trials of DHEA treatment effects on quality of life in women with adrenal insufficiency. J Clin Endocrinol Metab, 2009. 94(10): p. 3676–81.
36. Kallman, T.F., et al., The effects of opioid tapering on select endocrine measures in men and women with head and neck cancer — a longitudinal 12-month study. Pain Rep, 2024. 9(5): p. e1183.
37. De Nys, L., et al., The effects of physical activity on cortisol and sleep: a systematic review and meta-analysis. Psychoneuroendocrinology, 2022. 143: p. 105843.
38. Morales, A.J., et al., Effects of replacement dose of dehydroepiandrosterone in men and women of advancing age. J Clin Endocrinol Metab, 1994. 78(6): p. 1360–7.
39. Arinami, H., et al., Role of insulin-like growth factor 1, sex and corticosteroid hormones in male major depressive disorder. BMC Psychiatry, 2021. 21(1): p. 157.
40. Itodo, O.A., et al., Early changes in androgen levels in individuals with spinal cord injury: a longitudinal SwiSCI study. J Clin Med, 2022. 11(21): p. 6559.
41. Hu, Y., et al., Short-time intensive insulin therapy upregulates 3 beta- and 17 beta-hydroxysteroid dehydrogenase levels in men with newly diagnosed T2DM. Front Endocrinol (Lausanne), 2022. 13: p. 894743.
42. Chen, Y., et al., Meta-analysis of the association between sex hormones and pulmonary fibrosis. Postgrad Med, 2024. 136(5): p. 567–76.
43. Sultana, F., et al., Effect of dehydroepiandrosterone therapy on cognitive performance among postmenopausal women: a systematic review of randomized clinical trial data. Menopause, 2023. 30(11): p. 1167–73.
44. Mensión, E., et al., Safety of prasterone in breast cancer survivors treated with aromatase inhibitors: the VIBRA pilot study. Climacteric, 2022. 25(5): p. 476–82.
45. Mandal, S., et al., DHEA on sexual function in Sheehan Syndrome: a randomized double-blind placebo-controlled crossover trial. J Clin Endocrinol Metab, 2022. 107(8): p. e3395–402.
46. Weinland, C., et al., Sulphated dehydroepiandrosterone serum levels are reduced in women with alcohol use disorder and correlate negatively with craving: a sex-separated cross-sectional and longitudinal study. Addict Biol, 2022. 27(2): p. e13135.
47. McCrory, C., et al., Towards a consensus definition of allostatic load: a multi-cohort, multi-system, multi-biomarker individual participant data (IPD) meta-analysis. Psychoneuroendocrinology, 2023. 153: p. 106117.
48. Taylor, M.K., et al., Effects of dehydroepiandrosterone supplementation during stressful military training: a randomized, controlled, double-blind field study. Stress, 2012. 15(1): p. 85–96.
49. Salvini, S., et al., Effects of age, smoking and vitamins on plasma DHEAS levels: a cross-sectional study in men. J Clin Endocrinol Metab, 1992. 74(1): p. 139–43.
50. Swart, A.C., et al., The effect of soy isoflavones on steroid metabolism. Front Endocrinol (Lausanne), 2019. 10: p. 229.
51. Barton, D.L., et al., Evaluating the efficacy of vaginal dehydroepiandosterone for vaginal symptoms in postmenopausal cancer survivors: NCCTG N10C1 (Alliance). Support Care Cancer, 2018. 26(2): p. 643–50.
52. Moriguchi Jeckel, C.M., et al., Neuroendocrine and immunological correlates of chronic stress in 'strictly healthy' populations. Neuroimmunomodulation, 2010. 17(1): p. 9–18.
53. Binder, G., et al., Effects of dehydroepiandrosterone therapy on pubic hair growth and psychological well-being in adolescent girls and young women with central adrenal insufficiency: a double-blind, randomized, placebo-controlled phase III trial. J Clin Endocrinol Metab, 2009. 94(4): p. 1182–90.
54. Miller, K.K., et al., Androgens in women with anorexia nervosa and normal-weight women with hypothalamic amenorrhea. J Clin Endocrinol Metab, 2007. 92(4): p. 1334–9.
55. Kawano, H., et al., Dehydroepiandrosterone supplementation improves endothelial function and insulin sensitivity in men. J Clin Endocrinol Metab, 2003. 88(7): p. 3190–5.
56. Field, A.E., et al., The relation of smoking, age, relative weight, and dietary intake to serum adrenal steroids, sex hormones, and sex hormone-binding globulin in middle-aged men. J Clin Endocrinol Metab, 1994. 79(5): p. 1310–6.
57. Key, T.J., et al., Circulating sex hormones and breast cancer risk factors in postmenopausal women: reanalysis of 13 studies. Br J Cancer, 2011. 105(5): p. 709–22.
58. Koehler, K., et al., Low energy availability in exercising men is associated with reduced leptin and insulin but not with changes in other metabolic hormones. J Sports Sci, 2016. 34(20): p. 1921–9.
59. Fiedorczuk, P., et al., Potential diagnostic and monitoring biomarkers of obstructive sleep apnea — umbrella review of meta-analyses. J Clin Med, 2022. 12(1): p. 60.
60. Ruge, M., et al., Cross-sectional analysis of sleep hours and quality with sex hormones in men. Endocr Connect, 2019. 8(2): p. 141–9.
61. Ukraintseva, Y.V., et al., Slow-wave sleep and androgens: selective slow-wave sleep suppression affects testosterone and 17α-hydroxyprogesterone secretion. Sleep Med, 2018. 48: p. 117–26.
62. Brahimaj, A., et al., Serum dehydroepiandrosterone levels are associated with lower risk of type 2 diabetes: the Rotterdam Study. Diabetologia, 2017. 60(1): p. 98–106.
63. Zhang, X., et al., Low serum dehydroepiandrosterone is associated with diabetic kidney disease in men with type 2 diabetes mellitus. Front Endocrinol (Lausanne), 2022. 13: p. 915494.
64. Osei, F., et al., Association of primary allostatic load mediators and metabolic syndrome (MetS): a systematic review. Front Endocrinol (Lausanne), 2022. 13: p. 946740.
65. Qin, Y., et al., Effects of dehydroepiandrosterone (DHEA) supplementation on the lipid profile: a systematic review and dose-response meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis, 2020. 30(9): p. 1465–75.
66. Xie, M., et al., Impact of dehydroepiandrosterone (DHEA) supplementation on serum levels of insulin-like growth factor 1 (IGF-1): a dose-response meta-analysis of randomized controlled trials. Exp Gerontol, 2020. 136: p. 110949.
67. Nordmark, G., et al., Effects of dehydroepiandrosterone supplement on health-related quality of life in glucocorticoid treated female patients with systemic lupus erythematosus. Autoimmunity, 2005. 38(7): p. 531–40.
68. Jiménez, M.C., et al., Cardiovascular risk factors and dehydroepiandrosterone sulfate among Latinos in the Boston Puerto Rican Health Study. J Endocr Soc, 2018. 3(1): p. 291–303.
69. Arnal, P.J., et al., Effect of sleep extension on the subsequent testosterone, cortisol and prolactin responses to total sleep deprivation and recovery. J Neuroendocrinol, 2016. 28(2): p. 12346.
70. Lamon, S., et al., The effect of acute sleep deprivation on skeletal muscle protein synthesis and the hormonal environment. Physiol Rep, 2021. 9(1): p. e14660.
71. Wang, Z., et al., Effect of dehydroepiandrosterone administration before in vitro fertilization on the live birth rate in poor ovarian responders according to the Bologna criteria: a randomised controlled trial. BJOG, 2022. 129(7): p. 1030–8.
72. Mochón-Benguigui, S., et al., Sleep and anabolic/catabolic hormonal profile in sedentary middle-aged adults: the FIT-AGEING study. Int J Mol Sci, 2022. 23(23): p. 14709.
73. Akerstedt, T., et al., Adrenocortical and gonadal steroids during sleep deprivation. Sleep, 1980. 3(1): p. 23–30.


Related Content
What Can Lower Sex Hormone Binding Globulin? Is That Even A Good Idea?
Jun 15, 2026
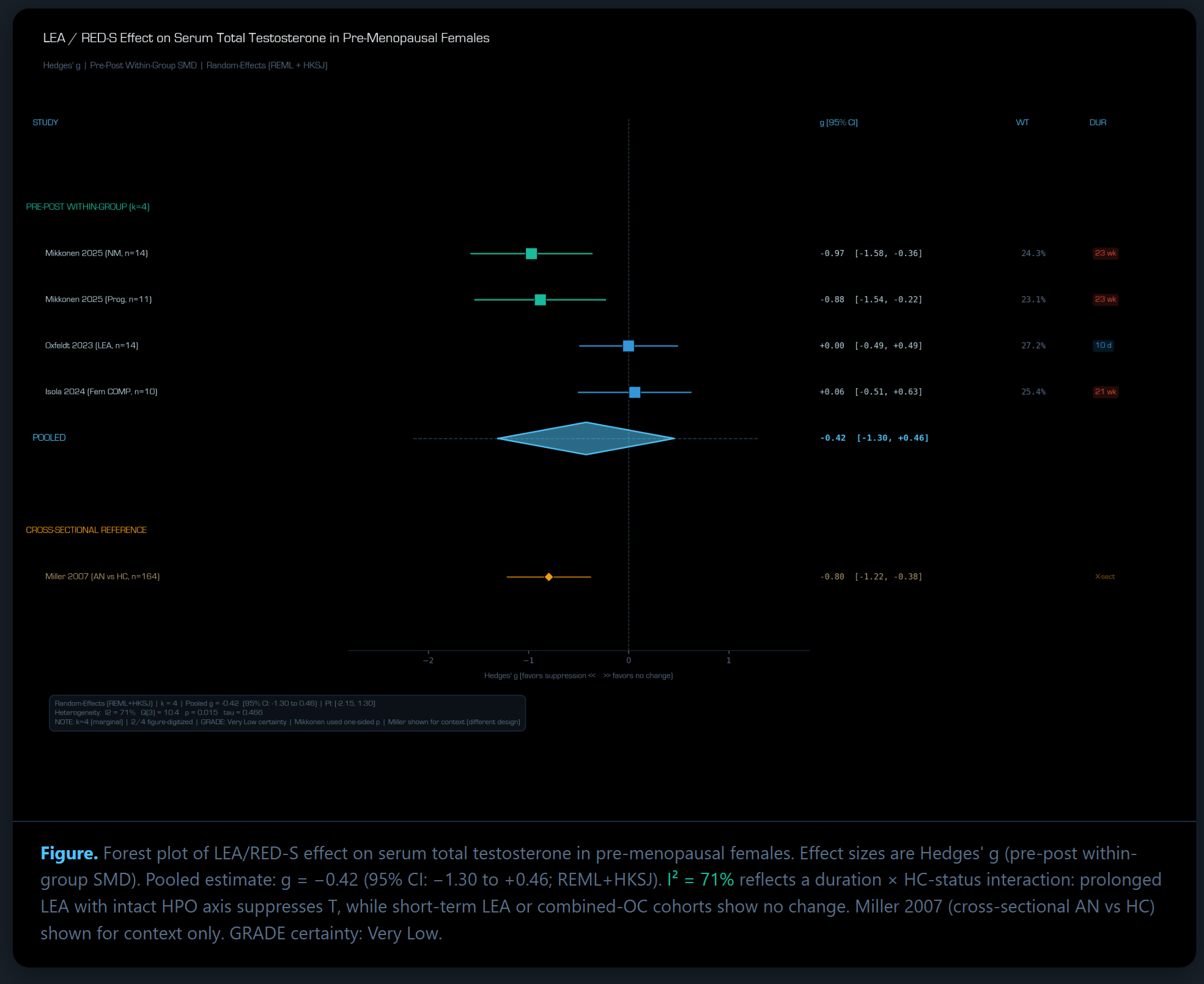
Does Low Energy Availability Affect Serum Testosterone In Females?
May 19, 2026
What Are Normal Testosterone, DHT, DHEA-S, and SHBG Levels Across The Menstrual Cycle?
Apr 30, 2026