

Below is a productive exchange with Dr. Gabrielle Fundaro that came about when we were preparing for Episode 146 of the Iron Culture podcast.
I also added a bit to this after the podcast to flesh out some ideas that I perhaps didn’t fully articulate on the episode.
Question One - Can Anti-Diet Culture and those who tread much more carefully with their tone on weight loss and “health” rally around a common enemy - the marketing techniques and strategies of diet culture and short-term fad fat loss?
Ben:
Pinterest recently banned this type of content (“the platform will no longer feature any advertisements that discuss weight loss, reference BMI, or show before-and-after imagery”) and Instagram says it is severely throttling this type of content down.
Marketers and pay-per-click teams are generally governed by metrics and capitalism.
They do what works.
They have their hammers and they slam them down as relentlessly as the metrics will allow them. But, over long time I think we can change the narrative and I hypothesize that the majority of the general population will eventually be somewhat disgusted by this type of short-term, aesthetic-based marketing from the weight loss side. I think humans will always like seeing sexy bodies…but sexy is obvie an individually and culturally subjective concept, and regardless I want everyone to feel sexy AF in their own body…right now with no strings attached.
One of the things that makes my skin crawl in this space is the expert creep from successful business individuals who inundate the nutrition and fitness world with their outcome-based, prestige-biased, clickbait, weight loss platitudes. Maybe it is time that we at least try to do the internal work to see that selling weight loss probably shouldn’t be the same game as selling vacuum cleaners.
These last two sentences may have ruffled some feathers and put some individuals guard up. It may have even come across as a personal attack.
“Empathy is an antidote to righteousness, although it’s very difficult to empathize across a moral divide.” -Dr. Jonathan Haidt
I also know those last few sentences come off as self-righteous on my part. But, please know that I have been the cringey Try Harder, What Gets Measured Gets Managed, weight loss coach. I have read more than my fair share of sales, business, and self-help books.
These books contain many useful tools and strategies, but a lot of those tools and their corresponding implicit narratives wielded blindly over short time periods in the body composition space are potentially dangerous.
I also understand the allure of this approach. I understand the financial, fame, and ego feed-forward cycle that these types of systems can build. I understand why it is easier to focus on objective markers and shock and awe changes, not only because people currently “like” them, but these numbers are what we can see and measure the most clearly (...maybe).
Yet, we have tried this personal responsibility objective weight loss game for the last 60-70 years and inside of our current built environment, it hasn’t really worked. Not only is obesity increasing, but body image issues are now becoming more pervasive across all BMI categories. Sure, we can survivorship bias our way into n of 1 stories where against all odds someone has made it work. But, the exception here kind of makes the “rule”.
Perhaps, it is time to think differently and reframe the narrative, and to objectively analyze what tools may be helpful, how could they be potentially deleterious, in who, at what time points, and for how long…
But, maybe you are just sick and tired of empathy and other people’s tired-ass feelings.
Maybe you believe empathy is an emotional contagion that clouds our ability to be objective and rationale on both the individual and group level.
To that, I say…SHOW ME THE DATA.
What’s the dropout rate of your intervention?
What's the likelihood of maintaining success at one year? Three years? Five?
What level of dietary restraint do subjects need to maintain those results? What is the cost of this in other aspects of their life?
If people fail what rationale or reasons do they give?
What long-term skills, resources, and competencies have these individuals acquired? Has their sense of self-efficacy and autonomy increased or decreased?
Are they better off metabolically? psychologically? If so, what is the effect size, and is it durable?
If you don’t have that data…I believe we can expect that at best at the group level the intervention may have made a slight difference over long time periods of time for weight loss and honestly, it could have even resulted in net weight gain compounded with more body image concerns if we bring in the drop-out data.
If you disagree with this hypothesis...maybe it's time to bring someone on like Dr. Fundaro to consult and help with the study design so that we can begin to answer these types of nuanced questions and decipher the cost-benefit ratios of these different tools and strategies.
That's my goal for 2022.
Gabi:
So much confusion stems from discussions that conflate dieting with weight loss and comparing cosmetic weight loss vs. weight loss for metabolic health.
People with overweight (OW) or obesity (OB) who are at risk of metabolic disease could use safer weight loss practices with a modest calorie deficit and perhaps maintain a small % weight loss long-term and experience improvements in metabolic health.
They could also use weight-neutral approaches and unintentionally lose weight, and still may experience similar improvements. Weight neutral approaches may not be as effective for improving physical health, but seem to pose less psychological risk.
People without OW or OB aren’t at foreseeable risk of metabolic disease, so intentional weight loss presents no clear benefits to physical health and other risk factors include: eating pathology = aesthetic reasons, appearance overvaluation, thin-ideal internalization, expectations of psychosocial benefits of thinness, body dissatisfaction, and in some cases increases in BMI (example: low BMI at the onset of dieting and adolescents with OW or OB at increased risk).
The anti-diet movement challenges diet culture, which encompasses intentional weight loss and often cites the harm of weight loss, conflating it with dieting (or intentionally reducing calories to lose weight).
Is the harm from WL? Not likely--it is more likely from the practices and reasons for pursuing WL and maybe from suppressing weight gain after it is lost.
Ben:
“People without OW or OB aren’t at foreseeable risk of metabolic disease.”
I would agree that the risk is less..., but I would heavily debate that people in the normal weight BMI category aren’t at increased risk for metabolic disease and this risk will depend on how you quantify metabolic health and track it over time [1]. Furthermore, the normal BMI category as it relates to metabolic disease risk is likely even more of an issue for those of Asian and Hispanic descent [1-3].
I would also argue that BMI is a fairly terrible place to start if we are looking for proxies of metabolic health, especially on the individual level. I debate this in somewhat more detail below, but only 20-30% of Americans in the normal BMI category would be considered optimally metabolically healthy, and to frame the nuance here is some NHANES observational data on prediabetes risk in the normal BMI category “The mean BMI for individuals without prediabetes was 22.2, and mean BMI for individuals with prediabetes was 22.6. The difference in means was statistically significant (P = .03). The mean waist circumference for individuals without prediabetes was 81.3 cm. For individuals with prediabetes, the mean waist circumference was 84.9 cm (P <.0001).” [4]
Thus, if someone has a lot of ectopic and visceral fat combined with a low amount of muscle mass the odds of being metabolic dysregulated are going to be higher no matter the BMI category they fall into [5, 6].
We talk about perhaps better ways to quantify body composition as it relates to metabolic health HERE, but we must remember that the best way to quantify metabolic health is to measure metabolic health!
So is weight loss making someone objectively healthier?
You can see the following fully referenced posts Is Weight Loss Impossible? and Can You Really Be Healthy At Any Size? and Is A Six-Pack Even Healthy?
Below I will speak to the potential physiologic effect of weight loss, diet, and/or exercise on objective metabolic health markers in the most relevant populations.
My main worry here from the metabolic health side is that we are lighting the fuse of chronic disease earlier and earlier so I am fairly confident that the prospective 0bservational research of boomers will be almost inapplicable to newer out the box generations. Getting a touch of Betes when you are 65+ doesn’t super scare me. Being diagnosed with overt Type 2 Diabetes when you are 25…that’s a lot eeek from a QoL, disability-free years, all-cause mortality, and economic standpoint.
“Men and women lost an average of 13.2 and 13.9 years from the age of diagnosis with diabetes.” -Salehidoost et al., 2020 [7]
What happens when we move that diagnosis earlier and earlier?
Want to get me riled up…talk about the CHILDREN!
“1 in 2 minorities born in 2000 will likely be diagnosed with diabetes.” [CDC]
“The prevalence of overweight and obesity among children and adolescents aged 5-19 has risen dramatically from just 4% in 1975 to just over 18% in 2016.” and over 51% have a waist that is greater than half their height [CDC and 29].
Children are 10 to 12 times more at risk for obesity when both their parents are obese [8].
Obese children are more likely than children with normal BMI to remain obese as adults and to experience greater risk of poorer health outcomes…early prevention during childhood is better than attempts at cure later in life.” -Bussiek et al., 2018 [9] (easyyyy with that word cure) and obese children likely have a 400% increased risk of T2DM when we only follow these individuals to age 25 [10].
Those in the normal weight BMI category at 18 had a lifetime T2DM risk of 17-20%, whereas in the overweight category the lifetime risk was 30-36%, and in the obese category it was 55 to 57%, and for those with a BMI over 35 at 18, the lifetime risk was 70 to 74% [1]. This paper was published in 2007 and my guess is that given the rise in childhood overweight and obesity these lifetime risk numbers will move up significantly in the coming decades.
#FoodSwamps and No Playgrounds....maybe a lack of competency, resources, social support, self-efficacy, skills, and autonomy are a big deal…
And here's the major rub...the Try Harder cognitive restraint diets aren’t really a viable standalone option in this population [11] and they very well could backfire [12, 13]!
Even telling children they are overweight or obese likely backfires [14, 15]. The only “thing” that seems to kind of move the needle in this population are multicomponent interventions [16]…Hmmmm maybe we have to hit the most massive “problem” of progress that our species has ever faced (not having to do physical labor and having easy and omnipresent access to delicious energy-rich food) from all angles…
No…no…no…we need 3-year-olds to be more personally responsible! No…no…no…of course not, we need their parents to Try Harder and be more responsible, except they too were likely some iteration of that same 3 year old.
Maybe we need to stop thinking about this problem in weeks and start thinking in generations.
I am not saying that personal responsibility isn’t part of the solution or that we as individual humans don’t have a responsibility to the group, but it is quite clear that shame and yelling at people to “Eat Less and Move More” isn’t effectively moving the needle.
But, is weight loss really healthy? Does everyone need to lose weight?
If we are going to talk about BMI, weight loss, and health we have to actually talk about objective metabolic health metrics, not just BMI.
Although BMI, is related to these metrics, the normal BMI absolutely does not automatically mean – Healthy…just like the Overweight and Obese categories don’t automatically mean Unhealthy. (I intentionally chose not to put the metabolic adjective in the above sentence.)
Araujo and colleagues found that across all BMI categories only 12.2% of Americans would be classified as having optimal metabolic health [17]. Dr. Tommy Wood and I reanalyzed the NHANES data with a bit tighter HbA1c criteria and it’s not pretty.
Stratified by BMI category and sex.
If a male is in the normal weight category, his likelihood of being metabolically healthy looks to be around ~20%. If he is in the overweight category, it drops to ~8.2%. If he is obese that number drops to just ~2.8%.
Females do fair better inside the current BMI breakdowns and below are the numbers:
If a female is in the normal weight category, her likelihood of being metabolically healthy looks to be around ~29.5%. If she is in the overweight category, it drops to ~15.1%. If she is obese that number drops to just ~7.3%.
The criteria we used for being categorized as metabolically healthy was: systolic blood pressure <120mmHg and diastolic blood pressure <80 mmHg; fasting glucose <100 mg/dL and hemoglobin A1c <5.5%; triglyceride <150 mg/dL, and a triglyceride to HDL ratio <2. We did not have medication data so these percentages are honestly probably even slightly lower and some people would want to take fasting trigs to under 100 mg/dL.
Now, let’s look at the scope of the problem from a purely metabolic disease standpoint. “People with diagnosed diabetes incur average medical expenditures of $16,752 per year, of which about $9,601 is attributed to diabetes. On average, people with diagnosed diabetes have medical expenditures approximately 2.3 times higher than what expenditures would be in the absence of diabetes.” The Cost of Diabetes - ADA [18]
According to NIH, an estimated 34.2 million people have diabetes (10.5 percent of the U.S. population).
· An estimated 88 million adults ages 18 years or older (34.5 percent of U.S. adults) have prediabetes.
· This includes nearly 29 million adults ages 18 to 44 years (24.3 percent of U.S. adults in this age group)
· more than 35 million adults ages 45 to 64 years (41.7 percent of U.S. adults in this age group)
· more than 24 million adults ages 65 or older (46.6 percent of U.S. adults in this age group.
· Among adolescents ages 12 to 18 years, more than 1 in 6 (18 percent of U.S. adolescents) have prediabetes.
The prevalence of prediabetes among adults in the US is around ~34% [19]. The annual progression from prediabetes to type 2 diabetes without any intervention is around 5 to 10% and a higher BMI, physical inactivity, and elevated fasting triglycerides all independently increase the risk of progression to type 2 diabetes [20, 21].
Depending on the definition for prediabetes, the risk of progression to type 2 diabetes is increased by 378 to 836% compared to those with normoglycemia [22].
Now let’s move the conversation to how effective weight loss can be at increasing or holding metabolic health and metabolic flexibility in those who are already on the spectrum of being metabolically unhealthy.
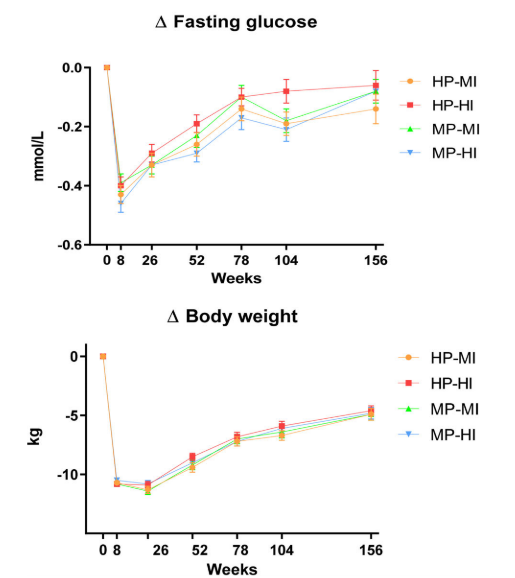
Let's start with PREVIEW by Raben et al., 2021 [23]. This study was done in a population with prediabetes and it resulted in an initial 11% weight loss and then roughly ~50% of that weight loss was maintained over three years. As you can see below, the metabolic health effects pretty much all flew with body fat loss and subsequent regain.
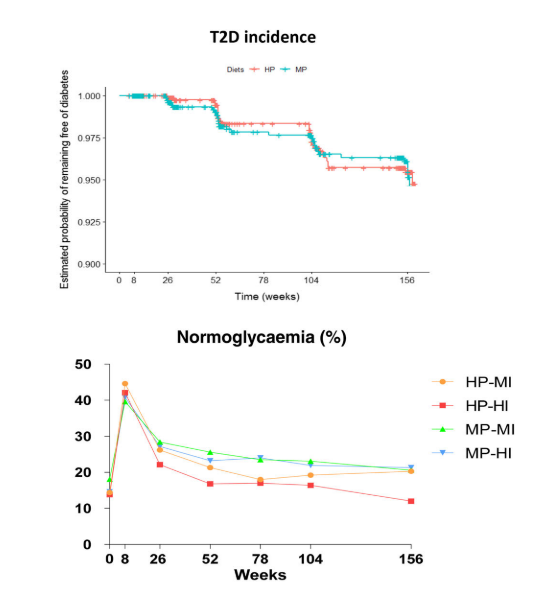
BUT, ONLY ~3% progressed from prediabetes to T2DM over three years [23]!!!!
That is a potential 500 to 1000% reduction in the progression from prediabetes to T2DM from this intervention (and it is possible that this risk reduction could be even more if you compared it to more at-risk populations).
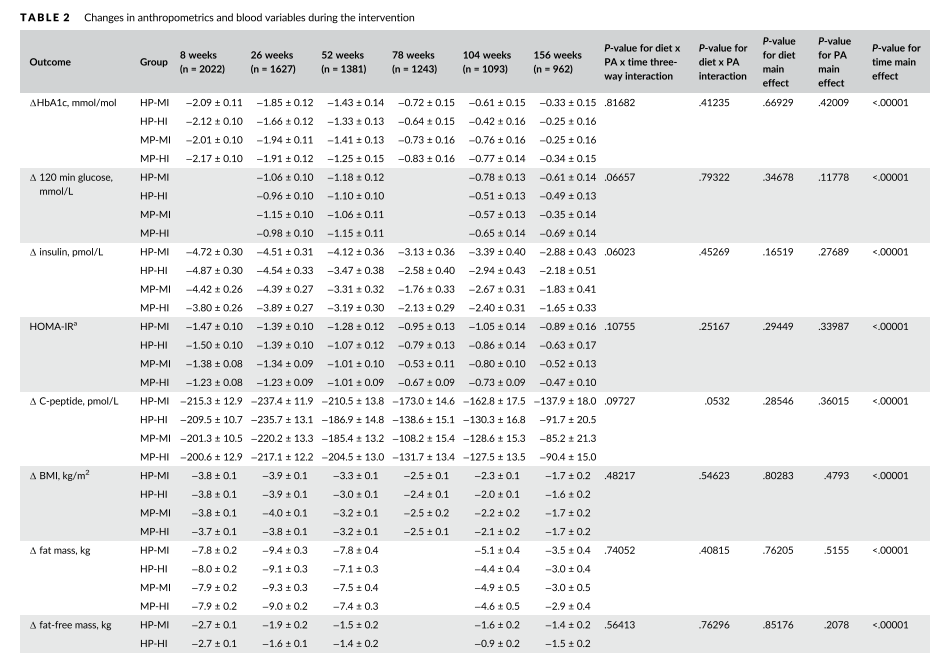
When we look at the table above we can see that every fasting metabolic health improvement parallels body fat loss and subsequent regain even with exercise and whole foods in the picture. I am sure people have bones to pick with the PREVIEW study design, but as far as interdisciplinary long-term weight loss studies go, it is one of the best ones we have to date.
Gabi:
It is also worthwhile to look at other metrics of health, and whether weight loss is necessary for improving QoL or body image (BI). Improvements in BI are temporary (so did it really improve or were positive scores higher because they were closer to their ideal? BI flexibility is probably more beneficial than positive BI). QoL is more impaired than improved in people seeking treatment [24].
Flourishing health = physical, psychological, semiotic, social ...is cosmetic WL supportive of health? What drives lower HRQoL in people with high BMI? Also, BMI relates differently to physical vs mental scores, and varies by age and sex [25].
(Some proponents might state otherwise, but the HAES.org --not Bacon’s book-- states that they don’t believe people are healthy at any size; rather, they deserve access to means for improving their health and focus on behaviors rather than outcomes)
One limitation of BMI and the argument against the Obesity Paradox is the lack of duration data--how long a person lived with OB. Perhaps spending less time with OB is beneficial even if it isn’t maintained. Data on the physical effects of weight cycling are inconsistent--but psychological effects may be harmful.
Odds of attaining normal body weight are also VERY low even for people with lower levels of OB:
“During a maximum of 9 years’ follow-up, 1283 men and 2245 women attained normal body weight. In simple obesity (body mass index = 30.0–34.9 kg/m2), the annual probability of attaining normal weight was 1 in 210 for men and 1 in 124 for women, increasing to 1 in 1290 for men and 1 in 677 for women with morbid obesity (body mass index = 40.0–44.9 kg/m2). The annual probability of achieving a 5% weight reduction was 1 in 8 for men and 1 in 7 for women with morbid obesity.” –Fildes et al., 2015 [26]
Ben:
Can we get wins in the beginning of the weight loss journey while immediately working on the behaviors and mindsets that are related to increases in autonomy and long-term success?
And getting results and meeting expectations to some degree in the beginning may be pivotal a part of this journey.
“A higher visit attendance was associated with greater weight-loss maintenance after 3 years. Further, PREVIEW used an LED for the first 8 weeks, which resulted in a large, rapid weight loss (−11%). This degree of weight loss appeared to be highly motivating for the participants as reflected in higher intentions for healthy eating, PA and self-efficacy, and a more positive perception about expected outcomes in those who had achieved target weight loss compared with those who had not.” [23]
Gabi:
I think this is compatible with a weight-neutral approach, which focuses on behaviors and mindset. This is important --if their motivation hinges on hitting their target weight loss, what happens when they reach maintenance? Or when they hit a plateau? IMO this is a disadvantage.
Anecdotally, most of my clients have been focused on WL for a long time, some even dieting from childhood. Though they may spend less time with OW or OB, the psychological costs are high. It seems to help more to focus on changing habits and letting weight do what it does for a while as they examine their current habits and decide what to replace.
Ben:
Why do we still think that set it and forget it weight loss is something that will be feasible for most people in our current obesogenic environment?
Why do we expect people to hit an everlasting weight loss grand slam on their first, second, or even third attempt? Why is this even the goal?
I’m not going to make anyone feel less than for how many times they have tried to lose fat and I am also not going to shame someone for still wanting that change in their body.
But, let’s try something different? Let’s work to align your values, processes, and outcomes. Not every strategy we use has to be sustainable, but if we all learn along the way, maybe we can find skills and strategies that ripple out into snowballing positives in our lives instead of just wanting to drop-kick the scale every morning.
Can we also just kill the shame of weight regain? (And maybe we can stop using the word weight loss recidivism or the tendency of a convicted criminal to reoffend). As to what Gabi said above, in certain populations that likely make up a large portion of the US (perhaps ~88 to 92% [17, 27-29]) by losing body fat even in weight neutrality we likely just significantly lowered their area under the curve from a metabolic disease standpoint.
What if we just reupped every once in a while with an active fat loss phase? How can we do this without the psychological downsides…is that even possible?
Recovery Diets back to a new energy balance and Mini Cuts with resistance training are tools that I don’t think we need to feel bad utilizing in the general population.
If we can lower the psychological cost of dieting to as little as possible and make the active fat loss phase as easy as possible while maintaining or gaining muscle and learning the skills of health…why not? Again, the answer here is nuanced and also likely psychology-related and very individual.
Now let’s go through some research in a novel population that shows this type of intervention may not be as “bad” as many in the healthosphere claim it to be.
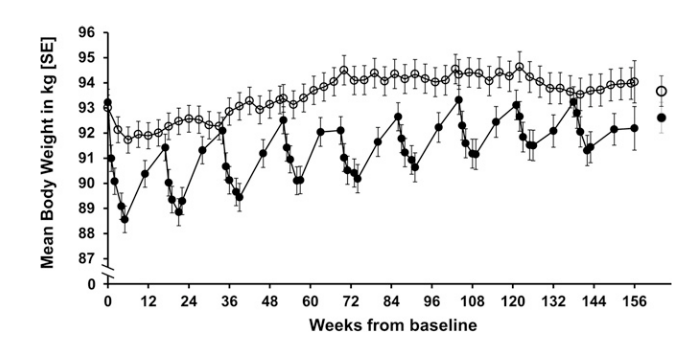
Open dots = one or two shakes per day fo eva eva “offered the use of 1–2 formula diet products daily throughout the 3 y, thereby reducing the daily energy intake by substituting 1–2 meals.”
Closed dots = 3 intensive weight loss periods per year, each lasting 5 weeks
People actually seem to like this meal replacement shake approach and the attrition rates in these studies tend to be fairly low, but we have to remember that we have significant QOL and pain changes in many of these types of weight loss studies [30-34].
To put the graph above into context, both groups started at around 104 kg and this is possibly the BEST long-term weight loss maintenance results we have to date with only roughly 20% of individuals gaining >5% weight gain at three years [30]. This is why the graph looks like it does, this particular study is a three-year follow-up after the CAROT study in subjects with knee osteoarthritis (KOA) who lost already ~13 kgs in 16 weeks from a previous intervention [35].
“Long-term obesity management with dietary approaches has generally been considered unsuccessful and a waste of time that, for most people, likely results in complete weight regain. Our results show only minor weight regain over 3 y and thus support the application of long-term meal replacement use and counseling, with comparable efficacy and safety of regular and intermittent strategies…. our study provides evidence against the concerns about weight cycling, which health care practitioners believe to be associated with untoward changes in body composition and increased cardiometabolic risk” -Christensen et al., 2017 [30]
To be clear, I don’t like that both groups in this study are still losing fat-free mass over three years, but this makes sense given there was no physical activity intervention, these individuals are likely even less active than the general population because of KOA, and the protein intake was probably a bit lower than we wanted. I also think that all of these physiologic downsides could be alleviated with one to two days of circuit training or resistance training per week and a bit more dietary protein.
Gabi:
The shame of weight regain may be derived, in part, from beliefs about body fatness and character. What does weight regain mean? Loss of control, lack of willpower, laziness, failure? Why? (Theoretically, fatphobia) Prior to 1910, body fatness was a sign of prosperity, but during WWI it was a sign of hoarding food. This is why the anti-diet community is challenging weight stigma and diet culture (which moralizes body size)...to remove the shame and stigma from body fat in general.
The psychological cost of dieting is high due to dietary restraint, especially in our current environment, and is perhaps also associated with preventing weight regain as opposed to maintaining weight in absence of weight gain [36].
Ways to reduce risk = focus on analysis instead of adherence, appropriate goals, self-compassion after setbacks, appropriate reinforcement of behaviors, health rather than aesthetic motives, and body image flexibility.
We also need to determine the reasons for weight gain--Knowledge gap? Sedentary lifestyle? Mood disorder? We may not need to focus on losing weight on purpose--What if we help people move more, eat more nutritious foods, and meet emotional needs effectively?
What about the general population fitness enthusiasts who are already healthy and constantly trying to maintain exceptionally low BF%?
Everyone is getting essentially the same message--weight loss is healthy and an achievement to pursue. No obvious net gain to more WL, just trying to avoid the shame of regain. Weight stigma and the morality of body size disproportionately affect people in large bodies, but it affects everyone IMO.
Ben:
Now let’s look at and reframe one of the largest and longest weight loss studies to date in those with Type 2 Diabetes.
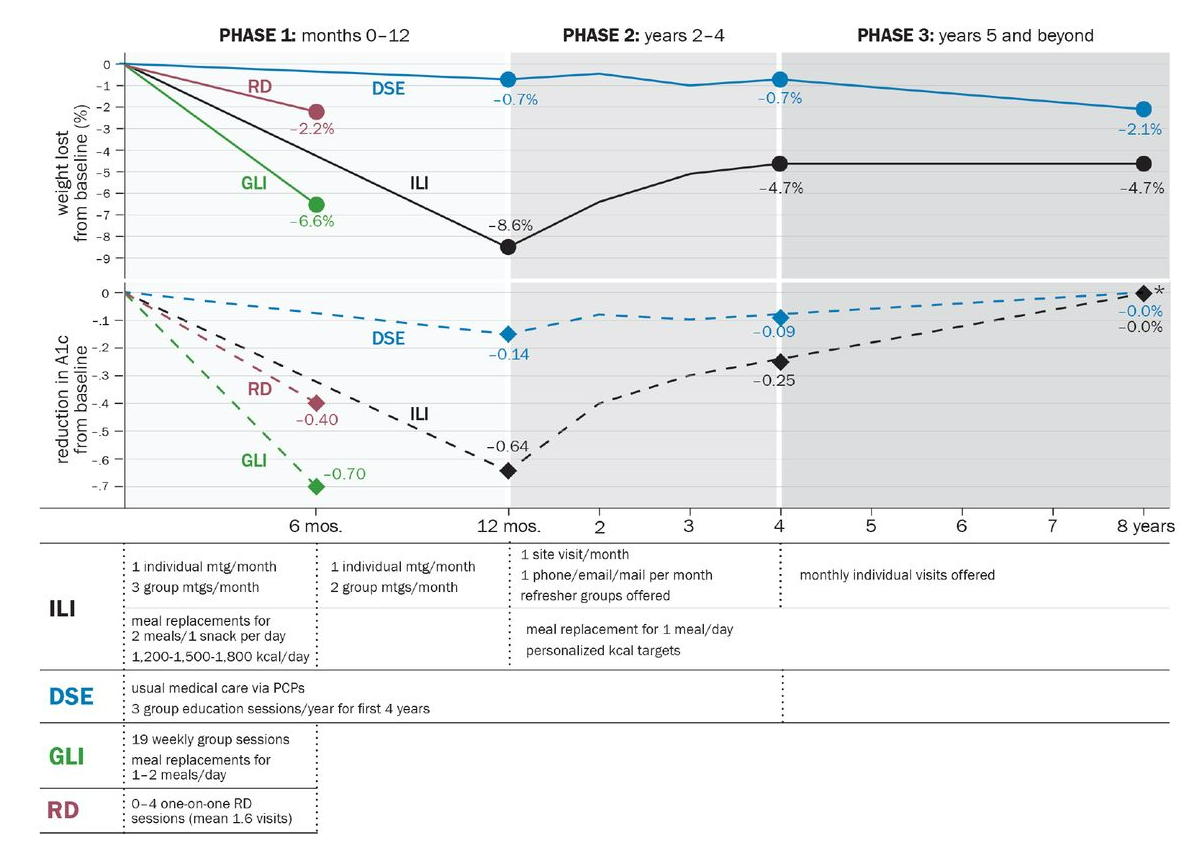
Above are the results from Look Ahead [37]
Again, a hunk of the narrative for this study is portrayed as a loss, BUT HbA1c didn’t go up after 8 years!! You can see the potential effect or lack thereof on disability-free years and all-cause mortality HERE. (I would hypothesize that this intervention started earlier in those with pre-diabetes would have vastly more positive effects for those same outcomes).
A quick breakdown of the results from the Look AHEAD study
N=5145 with T2DM
At 8 years
50% maintained ~5% Weight Loss
27% maintained ~ 10% Weight Loss
“Look AHEAD produced clinically meaningful weight loss (>/=5%) at year 8 in 50% of patients with type 2 diabetes and can be used to manage other obesity-related co-morbid conditions.” [38]
We need to acknowledge that America is phenomenal at losing the same ten to twenty pounds over and over again, and currently, ~65% of the US population are actively trying to lose weight or maintain weight loss [39]. A plethora of tactics and dietary strategies can result in substantial body composition changes within just four weeks [40, 41]. However, maintaining weight loss over the long term does look to be difficult with only around 20% of individuals maintaining 10% weight loss at one year [42], and without further interventions this number likely dwindles significantly over time with some estimates finding that over 95% those who lose weight gain it back after 3 to 5 years [43]. However, one of the fatal problems with the early diet and weight loss literature and one of the main foundations of the argument that weight loss is impossible comes from studies with no continued intervention or check-ins.
Gabi:
That begs the question--who can afford continued intervention and check-ins for...life? It’s both a limitation in the literature, but also a practical one. If they did receive continuous support, how well would that translate to public health interventions?
Ben:
Touche
Thus, is substantial long-term weight loss even possible?
Yes. [44-46] We know from the Look Ahead Study [38, 47] that, with continued monthly follow-ups, around 40% of those who lost 10% or more of their weight at one year, maintained that weight loss at year eight and 65% of this group maintained at least a 5% weight loss at year eight.
Gabi:
No argument here--but I wonder what the rates would be for cosmetic WL. A person who is already normative weight and loses 10% BW (pretty common in the 12-week transformations).
Ben:
Now let’s transition to Exercise Only Interventions in Prediabetes.
These interventions do seem to move the needle and thus may be able to arrest individuals in prediabetic testing values [48-54].
Yan et al., 2019 is the largest and longest prediabetes exercise study out of China. They saw small decreases in visceral adipose tissue (VAT), Fasting Glucose, and HbA1c…but saw no change in trigs or fasting insulin, so without significant body comp changes we are very likely not seeing durable changes in baseline metabolic health [53].
“After 12-month intervention, we observed that the incidence of diabetes was 8.6%, 5.7%, and 28.6% for one year in the AT, RT, and control groups, respectively. A significant difference in the number of prediabetes converted to diabetes was found in both aerobic and resistance training groups compared with the control group. This finding was consistent with the observation that the lifestyle intervention effectively reduced the incidence of diabetes. However, it was worth mentioning that the yearly diabetes conversion rate in the control group was higher in our study (28.6%) than those in the Da Qing (12.5%) and DPP studies (11%).”
Just to cherry-pick for fun - twice a week aerobic and resistance training with no dietary intervention may perform as well as metformin for increasing metabolic health [51].
BUT, without an energy deficit and subsequent body composition changes the effects of exercise are likely not durable past 24 hours [55-57] and that is OK!
Furthermore, the population in question is very important here as Exercise Interventions alone are very likely NOT making someone who is Type II Diabetic normoglycemic (maybe we get an average lowering of ~10mg/dL) [58].
If you mine the meta-analyses on this subject you find one massive outlier group. Cruz et al., 2019 [59].
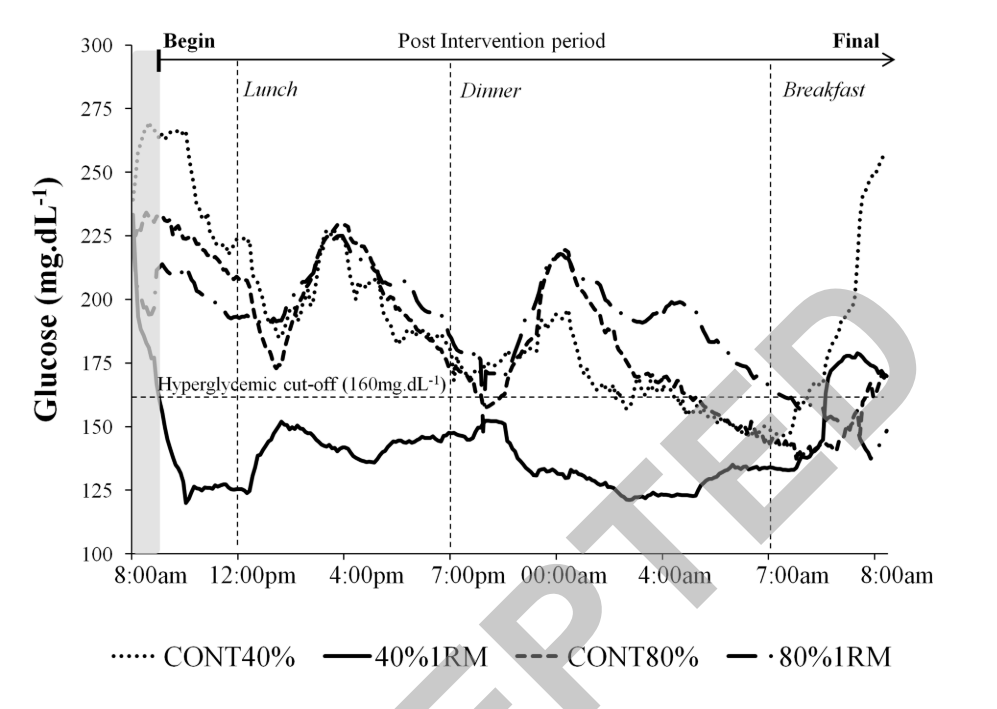
This 2019 cross-over study is absolutely amazing in that without any real type of dietary intervention low-weight high-rep circuit training was able to essentially push those with type 2 diabetes into the normal-ish glycemic range for 24 hours!
So it very likely isn’t possible to walk your way out of T2DM when someone remains in energy balance (doesn’t mean walking and movement can’t be really powerful), but someone may be able to circuit train their way into a semi-normoglycemic state with a lot of effort and that’s pretty cool!
Now, what about LOW LOW carb at energy balance?
Much to the surprise of many, extremely low carb diets in energy balance are probably not improving baseline metabolic health as much as many in the keto world think [60, 61].
You will likely limit post-prandial glucose spikes to a significant degree (at the potential cost of postprandial triglyceride spikes), but these extremely low carb interventions in energy balance are very likely NOT changing underlying metabolic health by a significant margin.
Gabi:
Also depending on perceived restriction/form of dietary restraint used to adhere to a keto diet, this could increase the risk of an eating disorder pathology.
Ben:
Let’s tie this all together.
Weight Neutral approaches very likely are not significantly moving the metabolic health needle [62, 63] or significantly changing dietary intake [64]. This isn’t really their intent anyways, BUT Weight Neutral approaches very likely may be able to arrest someone in their current metabolic health phenotype which is potentially a really really big deal for almost everyone living in our current modern built environment [65]!
Mixing weight neutral approaches as a way to maintain long-term weight loss is a bit odd from a semantics side, “but if it works…we’re right”? Weight neutral approaches seem to have the least downside from a psychology standpoint and thus these types of strategies may even be more applicable for individuals who may get the biggest bump in QoL and metabolic health from weight loss (i.e. those at risk for or on the diabetes spectrum and potentially those with chronic pain like KOA mentioned above) [30-33].
Gabi:
I absolutely agree, and it's a VERY careful conversation on mixing WN conversations with weight loss...which is why I call them 'universally applicable skills'
Ben:
Thank you Gabi for having this conversation and thank you to everyone who has read this far and is seeking to think about these questions in a more nuanced way.
REFERENCES:
1. Narayan, K.M., et al., Effect of BMI on lifetime risk for diabetes in the U.S. Diabetes Care, 2007. 30(6): p. 1562-6.
2. Gujral, U.P., et al., Diabetes Among Non-Overweight Individuals: an Emerging Public Health Challenge. Curr Diab Rep, 2018. 18(8): p. 60.
3. Teufel, F., et al., Body-mass index and diabetes risk in 57 low-income and middle-income countries: a cross-sectional study of nationally representative, individual-level data in 685 616 adults. Lancet, 2021. 398(10296): p. 238-248.
4. Mainous, A.G., 3rd, et al., Prevalence of Prediabetes and Abdominal Obesity Among Healthy-Weight Adults: 18-Year Trend. Ann Fam Med, 2016. 14(4): p. 304-10.
5. Gupta, P., et al., The Association between Body Composition using Dual energy X-ray Absorptiometry and Type-2 Diabetes: A Systematic Review and Meta-Analysis of Observational studies. Sci Rep, 2019. 9(1): p. 12634.
6. Taylor, R. and R.R. Holman, Normal weight individuals who develop type 2 diabetes: the personal fat threshold. Clin Sci (Lond), 2015. 128(7): p. 405-10.
7. Salehidoost, R., et al., Diabetes and all-cause mortality, a 18-year follow-up study. Sci Rep, 2020. 10(1): p. 3183.
8. Fuemmeler, B.F., et al., Parental obesity moderates the relationship between childhood appetitive traits and weight. Obesity (Silver Spring), 2013. 21(4): p. 815-23.
9. Bussiek, P.V., C. De Poli, and G. Bevan, A scoping review protocol to map the evidence on interventions to prevent overweight and obesity in children.BMJ Open, 2018. 8(2): p. e019311.
10. Abbasi, A., et al., Body Mass Index and Incident Type 1 and Type 2 Diabetes in Children and Young Adults: A Retrospective Cohort Study. J Endocr Soc, 2017. 1(5): p. 524-537.
11. Brown, T., et al., Interventions for preventing obesity in children. Cochrane Database Syst Rev, 2019. 7: p. CD001871.
12. Neumark-Sztainer, D., et al., Dieting and unhealthy weight control behaviors during adolescence: associations with 10-year changes in body mass index. J Adolesc Health, 2012. 50(1): p. 80-6.
13. Lowe, M.R., et al., Dieting and restrained eating as prospective predictors of weight gain. Front Psychol, 2013. 4: p. 577.
14. Robinson, E., et al., Telling people they are overweight: helpful, harmful or beside the point? Int J Obes (Lond), 2017. 41(8): p. 1160-1161.
15. Robinson, E., et al., Self-perception of overweight and obesity: A review of mental and physical health outcomes. Obes Sci Pract, 2020. 6(5): p. 552-561.
16. Gregory, J.W., Prevention of Obesity and Metabolic Syndrome in Children. Front Endocrinol (Lausanne), 2019. 10: p. 669.
17. Araujo, J., J. Cai, and J. Stevens, Prevalence of Optimal Metabolic Health in American Adults: National Health and Nutrition Examination Survey 2009-2016.Metab Syndr Relat Disord, 2019. 17(1): p. 46-52.
18. American Diabetes, A., Economic Costs of Diabetes in the U.S. in 2017. Diabetes Care, 2018. 41(5): p. 917-928.
19. CDC. Prevalence of Prediabetes Among Adults. 2020; Available from: https://www.cdc.gov/diabetes/data/statistics-report/prevalence-of-prediabetes.html.
20. Tabak, A.G., et al., Prediabetes: a high-risk state for diabetes development. Lancet, 2012. 379(9833): p. 2279-90.
21. Bennasar-Veny, M., et al., Lifestyle and Progression to Type 2 Diabetes in a Cohort of Workers with Prediabetes. Nutrients, 2020. 12(5).
22. Lee, C.M.Y., et al., Comparing different definitions of prediabetes with subsequent risk of diabetes: an individual participant data meta-analysis involving 76 513 individuals and 8208 cases of incident diabetes. BMJ Open Diabetes Res Care, 2019. 7(1): p. e000794.
23. Raben, A., et al., The PREVIEW intervention study: Results from a 3-year randomized 2 x 2 factorial multinational trial investigating the role of protein, glycaemic index and physical activity for prevention of type 2 diabetes. Diabetes Obes Metab, 2021. 23(2): p. 324-337.
24. Fontaine, K.R., S.J. Bartlett, and I. Barofsky, Health-related quality of life among obese persons seeking and not currently seeking treatment. Int J Eat Disord, 2000. 27(1): p. 101-5.
25. Apple, R., et al., Body mass index and health-related quality of life. Obes Sci Pract, 2018. 4(5): p. 417-426.
26. Fildes, A., et al., Probability of an Obese Person Attaining Normal Body Weight: Cohort Study Using Electronic Health Records. Am J Public Health, 2015. 105(9): p. e54-9.
27. Maffetone, P.B. and P.B. Laursen, Revisiting the Global Overfat Pandemic.Front Public Health, 2020. 8: p. 51.
28. Maffetone, P.B., I. Rivera-Dominguez, and P.B. Laursen, Overfat and Underfat: New Terms and Definitions Long Overdue. Front Public Health, 2016. 4: p. 279.
29. Maffetone, P.B., I. Rivera-Dominguez, and P.B. Laursen, Overfat Adults and Children in Developed Countries: The Public Health Importance of Identifying Excess Body Fat. Front Public Health, 2017. 5: p. 190.
30. Christensen, P., et al., Long-term weight-loss maintenance in obese patients with knee osteoarthritis: a randomized trial. Am J Clin Nutr, 2017. 106(3): p. 755-763.
31. Robson, E.K., et al., Effectiveness of Weight-Loss Interventions for Reducing Pain and Disability in People With Common Musculoskeletal Disorders: A Systematic Review With Meta-Analysis. J Orthop Sports Phys Ther, 2020. 50(6): p. 319-333.
32. Lean, M.E., et al., Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial.Lancet, 2018. 391(10120): p. 541-551.
33. Lean, M.E.J., et al., Durability of a primary care-led weight-management intervention for remission of type 2 diabetes: 2-year results of the DiRECT open-label, cluster-randomised trial. Lancet Diabetes Endocrinol, 2019. 7(5): p. 344-355.
34. Brown, A., et al., Low-energy total diet replacement intervention in patients with type 2 diabetes mellitus and obesity treated with insulin: a randomized trial. BMJ Open Diabetes Res Care, 2020. 8(1).
35. Christensen, P., et al., Comparison of a low-energy diet and a very low-energy diet in sedentary obese individuals: a pragmatic randomized controlled trial. Clin Obes, 2011. 1(1): p. 31-40.
36. Kruseman, M., N. Schmutz, and I. Carrard, Long-Term Weight Maintenance Strategies Are Experienced as a Burden by Persons Who Have Lost Weight Compared to Persons with a lifetime Normal, Stable Weight. Obes Facts, 2017. 10(4): p. 373-385.
37. Salvia, M.G., The Look AHEAD Trial: Translating Lessons Learned Into Clinical Practice and Further Study. Diabetes Spectr, 2017. 30(3): p. 166-170.
38. Look, A.R.G., Eight-year weight losses with an intensive lifestyle intervention: the look AHEAD study. Obesity (Silver Spring), 2014. 22(1): p. 5-13.
39. Santos, I., et al., Prevalence of personal weight control attempts in adults: a systematic review and meta-analysis. Obes Rev, 2017. 18(1): p. 32-50.
40. Longland, T.M., et al., Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: a randomized trial. Am J Clin Nutr, 2016. 103(3): p. 738-46.
41. Aragon, A.A., et al., International society of sports nutrition position stand: diets and body composition. J Int Soc Sports Nutr, 2017. 14: p. 16.
42. Wing, R.R. and S. Phelan, Long-term weight loss maintenance. Am J Clin Nutr, 2005. 82(1 Suppl): p. 222S-225S.
43. Langeveld, M. and J.H. de Vries, [The mediocre results of dieting]. Ned Tijdschr Geneeskd, 2013. 157(29): p. A6017.
44. Dombrowski, S.U., et al., Long term maintenance of weight loss with non-surgical interventions in obese adults: systematic review and meta-analyses of randomised controlled trials. BMJ, 2014. 348: p. g2646.
45. Natvik, E., et al., Living a successful weight loss after severe obesity. Int J Qual Stud Health Well-being, 2018. 13(1): p. 1487762.
46. Thomas, J.G., et al., Weight-loss maintenance for 10 years in the National Weight Control Registry. Am J Prev Med, 2014. 46(1): p. 17-23.
47. Dutton, G.R. and C.E. Lewis, The Look AHEAD Trial: Implications for Lifestyle Intervention in Type 2 Diabetes Mellitus. Prog Cardiovasc Dis, 2015. 58(1): p. 69-75.
48. Huang, L., Y. Fang, and L. Tang, Comparisons of different exercise interventions on glycemic control and insulin resistance in prediabetes: a network meta-analysis. BMC Endocr Disord, 2021. 21(1): p. 181.
49. Jadhav, R.A., et al., Effect of Physical Activity Intervention in Prediabetes: A Systematic Review With Meta-analysis. J Phys Act Health, 2017. 14(9): p. 745-755.
50. Wens, I., et al., High Intensity Aerobic and Resistance Exercise Can Improve Glucose Tolerance in Persons With Multiple Sclerosis: A Randomized Controlled Trial.Am J Phys Med Rehabil, 2017. 96(3): p. 161-166.
51. Malin, S.K., et al., Independent and combined effects of exercise training and metformin on insulin sensitivity in individuals with prediabetes.Diabetes Care, 2012. 35(1): p. 131-6.
52. Venojarvi, M., et al., Nordic walking decreased circulating chemerin and leptin concentrations in middle-aged men with impaired glucose regulation. Ann Med, 2013. 45(2): p. 162-70.
53. Yan, J., et al., Effect of 12-Month Resistance Training on Changes in Abdominal Adipose Tissue and Metabolic Variables in Patients with Prediabetes: A Randomized Controlled Trial. J Diabetes Res, 2019. 2019: p. 8469739.
54. Fritz, T., et al., Effects of Nordic walking on cardiovascular risk factors in overweight individuals with type 2 diabetes, impaired or normal glucose tolerance. Diabetes Metab Res Rev, 2013. 29(1): p. 25-32.
55. Ross, R., et al., Exercise-induced reduction in obesity and insulin resistance in women: a randomized controlled trial. Obes Res, 2004. 12(5): p. 789-98.
56. Schleh, M.W., et al., Energy Deficit Required for Exercise-induced Improvements in Glycemia the Next Day. Med Sci Sports Exerc, 2020. 52(4): p. 976-982.
57. Fisher, G., et al., Acute Effects of Exercise Intensity on Insulin Sensitivity under Energy Balance. Med Sci Sports Exerc, 2019. 51(5): p. 988-994.
58. Munan, M., et al., Acute and Chronic Effects of Exercise on Continuous Glucose Monitoring Outcomes in Type 2 Diabetes: A Meta-Analysis.Front Endocrinol (Lausanne), 2020. 11: p. 495.
59. Cruz, L.C.D., et al., Low-Intensity Resistance Exercise Reduces Hyperglycemia and Enhances Glucose Control Over a 24-Hour Period in Women With Type 2 Diabetes. J Strength Cond Res, 2019. 33(10): p. 2826-2835.
60. Hyde, P.N., et al., Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI Insight, 2019. 4(12).
61. Brown, A., et al., Dietary strategies for remission of type 2 diabetes: A narrative review. J Hum Nutr Diet, 2021.
62. Dugmore, J.A., et al., Effects of weight-neutral approaches compared with traditional weight-loss approaches on behavioral, physical, and psychological health outcomes: a systematic review and meta-analysis. Nutr Rev, 2020. 78(1): p. 39-55.
63. Ulian, M.D., et al., Effects of health at every size(R) interventions on health-related outcomes of people with overweight and obesity: a systematic review. Obes Rev, 2018. 19(12): p. 1659-1666.
64. Grider, H.S., S.M. Douglas, and H.A. Raynor, The Influence of Mindful Eating and/or Intuitive Eating Approaches on Dietary Intake: A Systematic Review. J Acad Nutr Diet, 2021. 121(4): p. 709-727 e1.
65. Mensinger, J.L., et al., A weight-neutral versus weight-loss approach for health promotion in women with high BMI: A randomized-controlled trial.Appetite, 2016. 105: p. 364-74.

Related Content
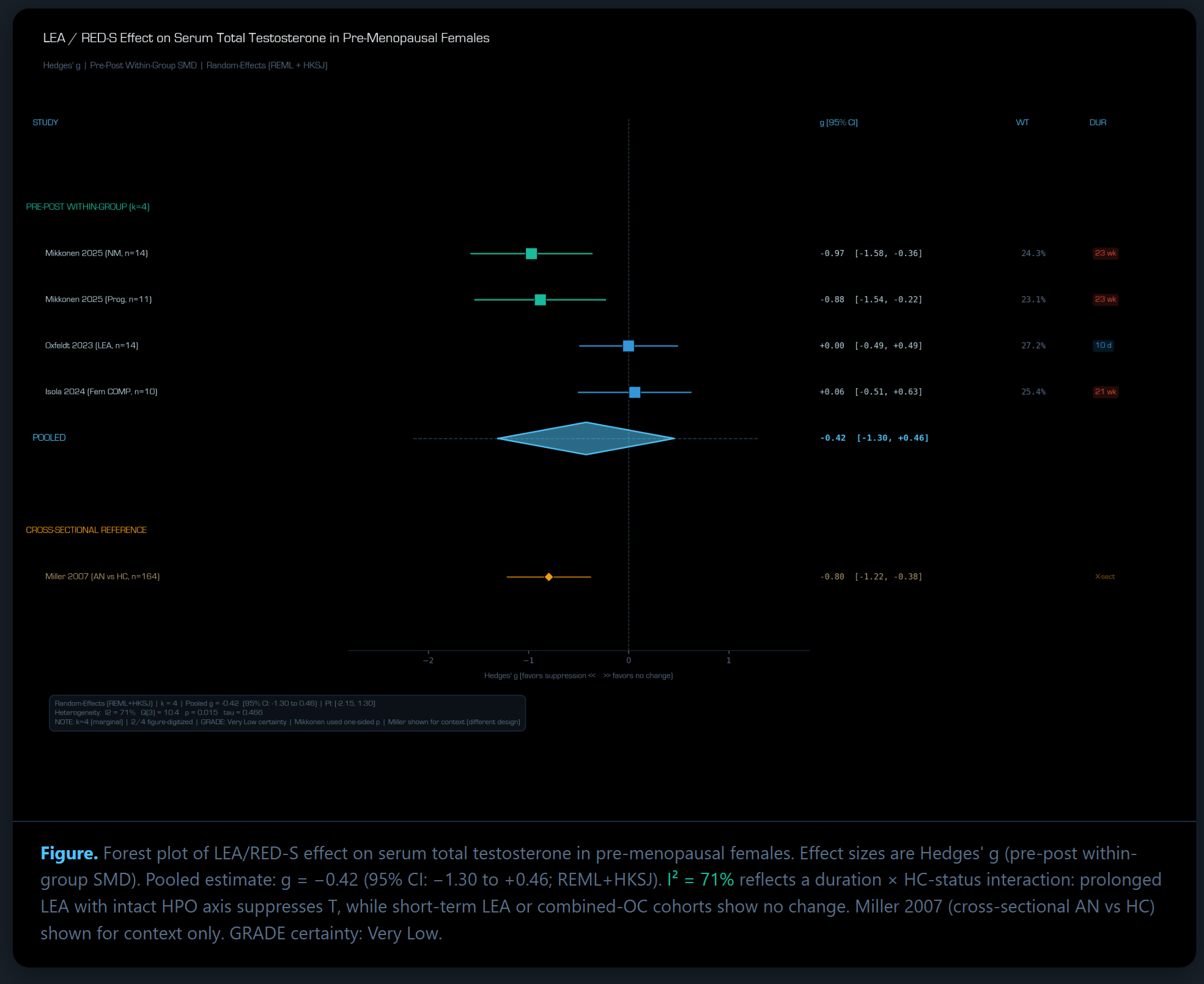
Does Low Energy Availability Affect Serum Testosterone In Females?
May 19, 2026
Can You Trust Bioimpedance To Measure Your Body Fat Percentage?
Mar 28, 2026
Revisiting Diet-Induced Muscle Loss.
Feb 14, 2026